
October 17, 2022
Note added November 4, 2022: On Nov. 3, 2022 initial results of the phase 2 study referenced in this post for psilocybin as a therapeutic for treatment-resistant depression have been published in the New England Journal of Medicine. The paper concludes: “In this phase 2 trial involving participants with treatment-resistant depression, psilocybin at a single dose of 25 mg, but not 10 mg, reduced depression scores significantly more than a 1-mg dose over a period of 3 weeks but was associated with adverse effects.” Larger and longer-term trials are urged by the authors.
IV. Neurochemical impacts of psilocybin and LSD
Hierarchical processing in the brain:
As we have described in other posts (see here and here), the human brain is a highly complex and highly integrated organ, in which a wide variety of sensory inputs from both the outside world and the internal organs of the body are continually received through a dense network of neurons and are processed and analyzed in several brain layers with gradually increasing precision. The brain’s interpretation of these inputs – i.e., the perceptions that they generate – is highly organized and guided by an individual’s prior experience and knowledge, starting with the rapid learning and brain “training” in infants.
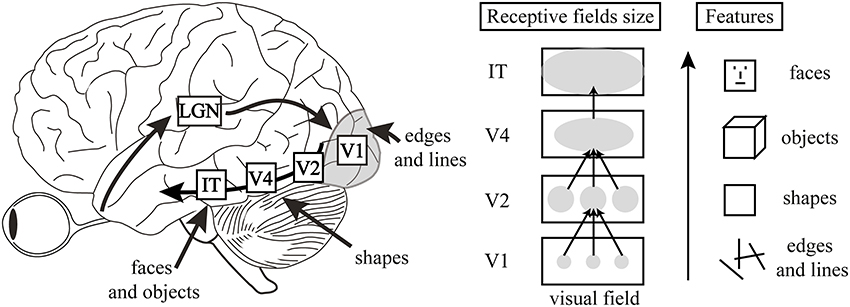
A widely accepted model for the successive levels of processing of sensory inputs in the brain was introduced in 1999 by computer scientists Rajesh Rao and Dana Ballard. Their model assumes a hierarchy of processing units, which, in the case of processing visual inputs, comprise a pathway that “begins in the retina, moves on to the lateral geniculate nucleus of the thalamus, and then to higher and higher levels of the cerebral cortex, named V1, V2, V4, IT, and onward.” Each level in this hierarchy makes predictions about the interpretation of activity in the level just below it and sends those predictions downward, while the level below sends an error signal upward if that prediction fails to account completely for the activity in the lower level. The generic sequence in forming perceptions is illustrated by Fig. IV.1, taken from an article by Harmer and Browning in the journal Biological Psychiatry.

An example of how this hierarchical visual processing proceeds is illustrated in Fig. IV.2. The lower levels of visual signal processing simply register that an object is seen, then provide some very basic information on orientation and shape. Only at the highest levels is the image identified with some particular type of object known from previous experience. In addition to perceiving known objects, those learned high-level predictions suppress hallucinations; for example, the human brain is trained to see faces, and sometimes we think at first that we may see them in objects such as trees, mountains, clouds, or even pieces of toast, but experience contained in the high-level predictive layers of the brain tells you that these objects do not contain faces. This organization of the brain is essential for an individual to function reasonably in a world full of stimuli. On the other hand, a variety of psychological disorders appear to be caused by an overweighting in the brain of pathological or maladaptive learned beliefs and consequent predictions.
The experience of hallucinations under the influence of psychedelic drugs would then be expected to result from a weakening in some way in this chain of predictions based on prior experience. Friston and Carhart-Harris refer to this weakening by the acronym REBUS, standing for RElaxed Beliefs Under pSychedelics. If overweighted maladaptive beliefs in someone suffering from psychological disorders such as depression or excessive anxiety can be relaxed, or even broken down, under controlled psychedelic treatments, then one might expect useful therapeutic applications in treating some mental diseases, such as those indicated in Fig. IV.3.

Psychedelics and serotonin receptors:
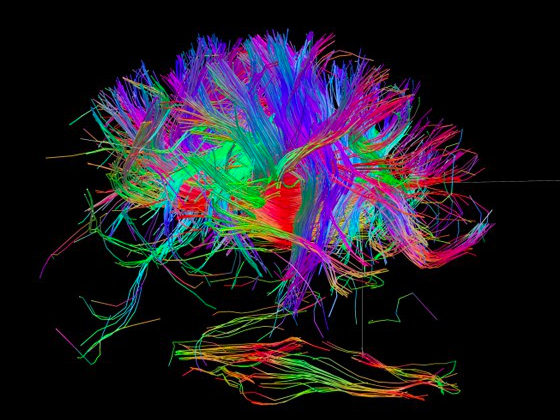
How does this relaxation of beliefs under psychedelics occur neurochemically? The signals from sensory organs to the brain, and among the various parts of the brain, are carried along the dense network of neurons pictured in Fig. IV.4. Those signals are transmitted across the synaptic gaps in neuronal paths by several different neurotransmitter chemicals. We have described the role of one such neurotransmitter, dopamine, in our previous post on Brainwashing via Social Media.
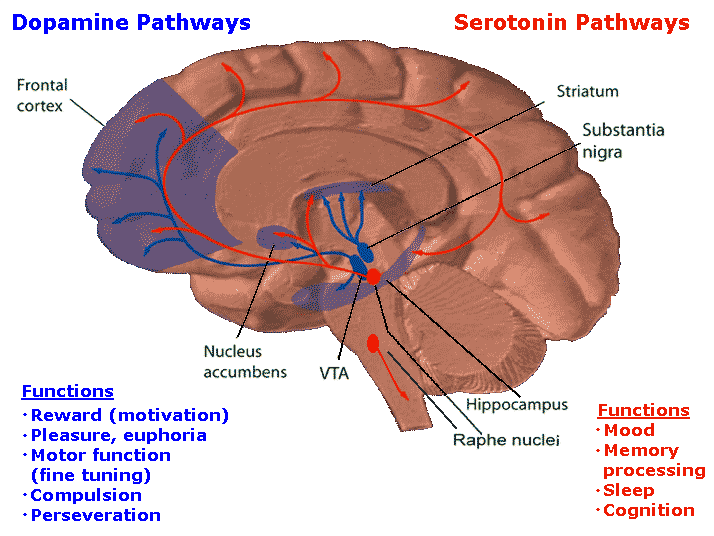
The neurotransmitter most associated with the impacts of psychedelics on the brain, as well as with various psychiatric disorders when its levels are too low or too high, is serotonin. As illustrated in Fig. IV.5 in comparison with dopamine pathways in the brain, serotonin pathways connect to a wider array of brain regions, especially to outer layers of the cerebral cortex involved in cognition, learning and high-level perception formation, though both chemicals transmit signals to the prefrontal cortex that acts as the brain’s highest processing level. Serotonin thus affects a diverse range of human physical and psychological functions, including brain development, mood, digestion, memory processing, sleep, cognition, sexual function, and bone health. Abnormal serotonin levels appear to be correlated with such psychological disorders as depression, anxiety, sleep disorders, panic disorders, schizophrenia, and various phobias.
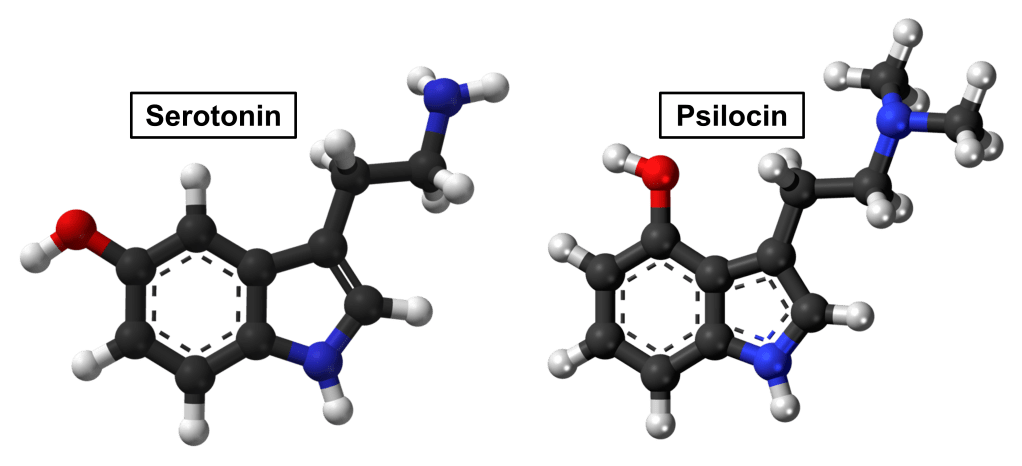
The chemical structure of serotonin is compared in Fig. IV.6 to that of psilocin, the chemical formed from the psilocybin in magic mushrooms when it undergoes hydrolysis inside the body’s gastrointestinal tract. The striking similarity between the two chemicals is at the heart of the effect of psychedelics on the brain. When serotonin (known chemically as 5-hydroxytryptamine, or 5-HT for short) is emitted by a sending neuron, it is received across synaptic gaps by specialized receptors distributed throughout the brain. The particular receptors distributed densely throughout the cerebral cortex are labeled as 5-HT2A. Those same receptors can be activated by psilocin, so that a psilocybin or LSD (with somewhat similar chemical structure) “trip” affects the brain in a similar way as a dramatic change in serotonin signaling in the cerebral cortex.
The central role of the 5-HT2A receptors has been demonstrated in research using the drug ketanserin to block the activation of these receptors. For example, animal research has shown that chemically blocking 5-HT2A receptors makes rats “cognitively inflexible: They are no longer able to spontaneously change from one behavior to another in order to get a reward. In the context of predictive processing [see Fig. IV.1], the finding suggests that the 5-HT2A-blocker made the rats’ brains more tightly constrained by prior beliefs about the world.” Conversely, one might expect overstimulation of the 5-HT2A receptors, as in psychedelic trips, may reduce the influence of prior learning and high-level predictions in guiding the brain’s formation of perceptions, making it more susceptible to hallucinations and unusual connections. In studies carried out by the Zurich group under Preller and Vollweider, they indeed found that using ketanserin to block 5-HT2A receptors along with delivery of LSD to subjects strongly attenuated the hallucinogenic effects of the drug.
Psychedelics rewire the brain’s network connections:
The Imperial College group has carried out a series of brain imaging studies of volunteer subjects injected with either psilocybin or LSD. The revealed effects of the two drugs are quite similar, although the two drugs differ substantially in potency. LSD has a greater affinity to stick to the 5-HT2A receptors, hence, its effects set in at considerably lower doses than those of psilocybin. The studies have used all three imaging techniques mentioned in Part I, fMRI, EEG, and MEG. The results of these studies have been nicely summarized by Carhart-Harris in two detailed invited talks (given some nine years apart), available here and here on YouTube, on which we rely heavily in the following descriptions. Because observations with the two drugs and the three imaging techniques all seem mutually consistent, we only summarize a small set of the highlights from studies of either drug here.
In order to understand how psychedelics affect connections within the brain, one should start with some understanding of connections in an unaffected brain. Brain activities tend to involve networks of several brain regions connected by subsets of the full neuron connectome. Imaging studies on normal human brains have revealed the existence of a Default Mode Network (DMN) comprising the brain regions and neural connections among them that are continuously active as a baseline “rest” mode, even when an individual is not focused on any particular mental task or interaction with the outside world. The DMN was discovered in studies by Marcus Raichle and collaborators at the Washington University School of Medicine, who also showed that the brain’s energy consumption is increased by less than 5% of its baseline default mode energy consumption when it focused on a specific mental task. The regions of the brain involved in the DMN are illustrated in the fMRI scan shown in Fig. IV.7: the medial prefrontal cortex, the posterior cingulate cortex, and the angular gyrus, with the posterior cingulate cortex acting like a transit hub hosting a large number of neural connections, as revealed in the DMN connectome shown in Fig. IV.8.


It has been shown that the DMN is activated, for example, when an individual is engaged in self-reflection, the formation of complex mental images, daydreaming, thinking about the past or the future, or thinking about the nature of thinking itself. Raichle has thus hypothesized that the DMN is the “orchestrator of the self.” In patients suffering from depression, when they are deeply engaged in obsessing about themselves and their own problems, the connections between the fore and aft regions of the DMN are especially strongly activated.
It is speculated that the DMN plays the role of a “central orchestrator or conductor of global human brain function.” In this picture, the default mode network acts like a “reducing valve” for information from the outside world. In this theory, the DMN has evolved to restrict the amount of outside information that is processed by the brain. This helps to ensure that competing signals from one brain network do not interfere with signals from another network. The net result is that the DMN makes the brain more efficient in dealing with the outside world, and with making rational assessments of reality.
Imaging of brains on psilocybin or LSD has revealed that the DMN is significantly weakened while, in the reduced presence of this normally dominant baseline, alternative, seldom activated, connections are strongly enhanced, dramatically altering the brain’s sense of self and the high-level predictions that normally tightly restrict the formation of perceptions.
For example, in one experiment Carhart-Harris’ group performed fMRI scans on a set of 15 healthy volunteers at rest after they were given moderate dosages (2 mg) of psilocybin and, in a separate run, of a placebo, in both cases intravenously. When the drug is delivered intravenously its effects begin quite rapidly, typically within 60 seconds of the start of the delivery. The scans allowed them to observe changes in cerebral blood flow and in oxygenation between the psilocybin and placebo trials, as a function of location within the brain. What they observed systematically (see Fig. IV.9) was a clear decrease in blood flow and oxygenation to the cortical regions involved in the DMN when the subjects had received psilocybin. The magnitude of the decrease tended to grow in size with the intensity of the psilocybin “trip” self-reported by the subjects. Corroborating effects have also been observed with EEG and MEG analyses.

The fMRI scans also allow one to map out the time response of various brain regions and to identify the regions that are functionally connected, i.e., activated in sync as part of a network – such as the medial frontal cortex and the posterior cingulate cortex in the DMN in normal brains – as well as those regions not involved in such a network, as their activity is out of sync. Figure IV.10 shows the dramatic changes in the networks responding to visual stimuli between a brain on a placebo (on the left) vs. one on LSD (right).
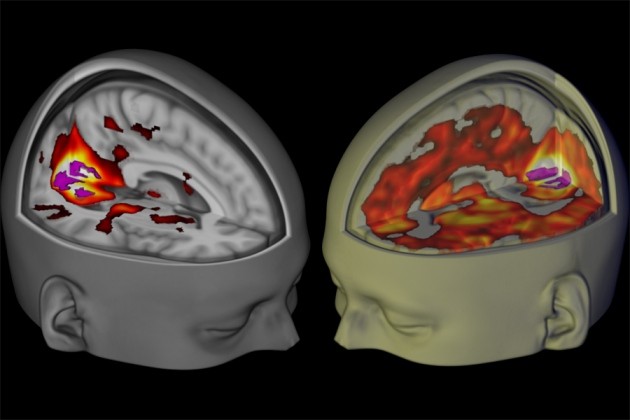
The intensely activated region at the rear of the brain in both images in Fig. IV.10 is the primary visual cortex (V1 in Fig. IV.2). In the brain on placebo, V1 is activated in sync with the other regions of the visual predictive hierarchy indicated in Fig. IV.2. But on LSD, extensive regions of the cortex, not normally involved in visual processing, are excited in sync with the visual cortex, suggesting that one may have escaped the usual predictive visual processing described earlier and entered a regime where the visual perceptions are no longer guided by learned reality. Furthermore, the perceptions under LSD can be triggered with eyes closed, that is, without external stimulation of V1. This is then the scan equivalent of the vibrant hallucinations and sensory anomalies that subjects on psychedelics report, sometimes with claims that they could see smells, taste colors, feel sounds, etc.
This dramatic expansion of functional connectivity of essentially the entire cortex on psychedelics is not limited to just the visual network but appears to affect most brain function. This has been illustrated schematically in the network figure IV.11, where dots along the circumference effectively represent brain regions, color-coded by the networks to which they normally belong. The curves joining various dots represent the functional connections. On psychedelics the brain becomes “hyperconnected,” with connections excited among diverse brain regions that normally do not activate in sync with one another. This hyperconnectedness could be the brain activity manifestation of the “mind (or consciousness) expansion” trippers often report.

Another qualitative report of the somewhat mystical experience subjects feel on psychedelics is a sense of “oneness” with the outside world. Carhart-Harris reports, for example, that one subject put it this way: “The feeling of no boundaries, I did not know where I ended and my surroundings began. Somehow I was able to comprehend what oneness is.” This feeling appears to be another manifestation of the hyperconnectedness of the brain on psychedelics. In Fig. IV.12, Carhart-Harris shows that in the normal brain, activation of networks associated with perceptions of outside objects (colored here in shades of blue) is completely out of phase (as a function of time) with the DMN (colored in yellow, orange and red) that provides the sense of self; these networks are normally in competition, when one is activated the other is not.

On psychedelics, however, this competition disappears: as the DMN, the supposed “orchestrator of the self” is suppressed and the brain becomes hyperconnected, inward- and outward-looking networks show up as fleetingly and randomly, but often simultaneously, activated. They become part of one overall, hyperconnected, but also “disordered,” brain network. This could explain why the clean distinction between self and other fades away. Without psychedelics, that sort of loss of boundaries of the self occurs primarily in mental illness, such as schizophrenia.
Entropy in brain function:
The results of the Imperial College neuroimaging studies, together with other studies of brain function, have led to a model regarding the function of the brain. This model adapts the concept of entropy from the field of physics, where it provides a quantitative measure of the degree of disorder within a system. A system that is highly ordered has low entropy, while a more chaotic system has higher entropy. For example, a system of atoms where every atom occupies the same quantum state will have low entropy, while a system where the atoms may occupy any among many different quantum states will have a higher entropy. As applied to the human brain, this concept is reviewed in the paper The Entropic Brain: A Theory of Conscious States Informed by Neuroimaging Research with Psychedelic Drugs, by Carhart-Harris, et al.
In the entropic brain model, the default mode network plays a key role in determining the “normal” state of waking consciousness. In this state, various areas of the brain operate somewhat autonomously. Connections between different brain regions are minimized, and brain waves in different regions tend not to be correlated with one another. In this theory, the optimal normal waking state corresponds to a “sweet spot” of moderately low entropy, as suggested in the entropy spectrum shown in Fig. IV.13. This organization enables the individual to interact effectively with the outside world, and the individual also maintains a clear sense of ‘self;’ in this sense, Carhart-Harris and associates posit that the DMN provides the neurological basis for the self (or, in psychoanalytic terms, the ego).

The DMN is responsible for regulating the traits of self-reflection, recalling the past and speculating on the future. These traits are possessed at a much higher degree in adult humans; they are not strongly expressed by other primates or even by human infants, whose brains are not yet fully developed. In the entropic brain model, the modes of thinking that characterize infants and non-human primates are called primary consciousness. The adult human state of waking consciousness, where individuals possess the capacity for self-reflection and act ‘rationally,’ is referred to as secondary consciousness. Compared to primary consciousness, the secondary consciousness that defines the normal waking states of a fully developed human brain is a state of relatively low entropy, where the DMN helps to organize the brain into “coherent, hierarchically-structured systems” that enable the individual to process its environment as precisely as possible, with minimal uncertainty. In the higher-entropy states of primary consciousness an individual accesses many novel mental perceptions, some of which may appear to normal adult humans as bizarre or senseless.
Toward the high-entropy end of the spectrum in Fig. IV.13 one finds conditions of highly disordered brain function and often random perceptions, unconstrained by reality, that characterize schizophrenia or early psychosis, as well as dreaming and near-death experiences. Also in this category is “magical thinking,” where the individual adopts supernatural interpretations of phenomena. Magical thinking tends to be more common in circumstances of high uncertainty, thus it corresponds to a state of higher entropy in this model. Under conditions of severe stress or sensory deprivation, even healthy humans may regress to the high-entropy states of primary consciousness. And it is clear from the neuroimaging results of Carhart-Harris and collaborators (see here, here and here) that the hyperconnectedness induced by psychedelics corresponds to a temporary, but significant, increase in entropy of the human brain.
Neuroimaging experiments have shown that the administration of psilobycin or LSD shifts brain behavior from the relatively low-entropy state of normal brain activity to a more chaotic state associated with higher entropy. Young children, people engaged in “magical thinking” and people with schizophrenia also experience more disordered, higher-entropy states of brain function. However, it is important to note that at present, we do not know whether these different states are related to one another and/or how similar these different states may be. All this is dependent on the results of future studies of brain neurochemistry.
There are also psychiatric disorders that fall near the low-entropy end of the spectrum. For example, persons experiencing depression or compulsions are likely to be obsessive in reflecting on past negative experiences or self-perceptions, or they may be fearful of future events. Their capacity for self-reflection results in a rigidity of mind, a mental rut, often leading to self-destructive behavior. Other conditions characterized by low-entropy, inflexible mental processes can be spurred by addictions or by extreme anxiety arising from health concerns. The interest in potential therapeutic uses of psilocybin and LSD, surveyed in the next section, arises from the hope that psychedelic jolts leading to increased entropy states may help to boost the brain out of these self-destructive low-entropy states, perhaps even with some permanence.
V. clinical studies of psilocybin- and lsd-assisted psychotherapy
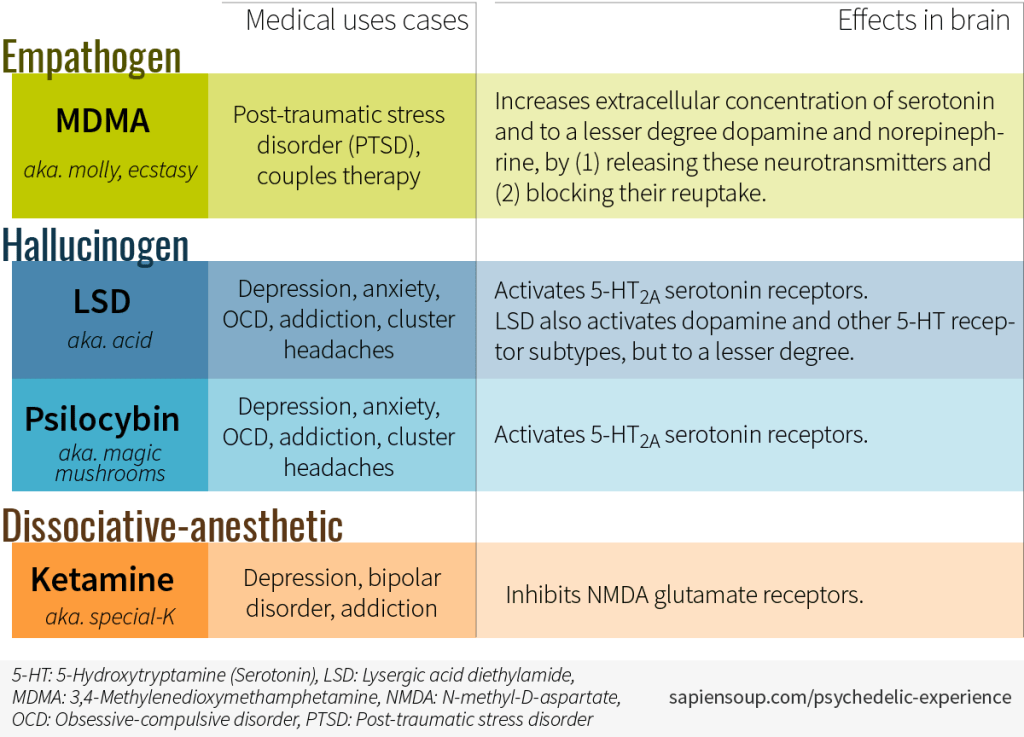
The tendency of psychedelics to increase the brain’s degree of disorder is what has spurred ongoing trials to see if psychedelics can be used to “unlock” the inflexible and self-defeating brain networks that cause such illnesses as depression, anxiety, obsessive-compulsive disorder (OCD), and addiction. The therapeutic hope is based on the concept of neural plasticity, that is, the idea that neural networks can be retrained with some permanence after a relatively short treatment plan coupling psychedelics with more traditional psychotherapy. On the other hand, application of psychedelics might enhance any predisposition to high-entropy psychosis in some subjects. The table in Fig. V.1 indicates the disorders to which psilocybin and LSD are currently being applied to carefully screened volunteers, as well as applications of two other psychedelic drugs that have different mechanisms for their brain impacts.
There was an active program of LSD- and psilocybin-based therapy for anxiety, depression, and addiction during the 1950s to about 1970, prior to the classification of psilocybin and LSD as Schedule I drugs. While some of these early studies provided hints of potential therapeutic uses, few of them were carried out according to the randomized and placebo-controlled large-sample standards that would be required today for government approval of a therapy. According to an article in the Psychiatric Times, “The pharmaceutical company Sandoz ceased LSD and psilocybin manufacturing in 1965, and in 1970, the Controlled Substances Act placed psilocybin, LSD, and other psychedelic drugs under the Schedule I designation. This action resulted in a cessation of research associated with these agents. The revival of research into psilocybin and LSD began 25 years later under strict restrictions, when preliminary findings displayed promising results for a variety of psychiatric disorders. In the past several years, there have been more research studies on psychedelics than at any previous time…In 2018, the FDA designated psilocybin for TRD [treatment-resistant depression] and 3,4-methylenedioxymethamphetamine (MDMA)-assisted psychotherapy for posttraumatic stress disorder (PTSD) as breakthrough therapies.”
However, the continuing Schedule I designation for psilocybin and LSD in both the U.S. and U.K. restrict access to federal funding for research on the drugs’ effects. Furthermore, the large pharmaceutical companies see little profit motive for funding large-sample clinical trials: these drugs already exist, are not patentable, and the envisioned treatments involve delivery of only a small number of doses. Thus, ongoing clinical trials have been privately funded and they involve relatively small subject samples, without ideal control group matches.
In addition, these trials face unique challenges. As mentioned in Part I, it is extremely difficult to perform “double-blind” experiments with patients, as there are essentially no non-psychedelic substances that produce the same effects as psychedelic drugs without activating the serotonin receptors. Both subjects and administrators of any trial can clearly discern whether the psychedelic drug or a placebo has been used. Furthermore, the pre-1970 trials had already established that the effect of the drug is significantly dependent on both the state of mind of the participants before they take the drugs and the environment in which the drugs are given – these are now referred to as the “set and setting” for the psychedelic experience. It is not easy to make meaningful comparisons among trials carried out with dissimilar sets and settings or different drug dosages.
And even with set and setting for a treatment trial controlled, the effects of psychedelics can vary widely from one event to another. Sometimes psychedelics can produce a “bad trip,” where the user may experience a panic attack or other serious negative side-effects. Researchers who have overseen drug trials with psilocybin and LSD report that it is relatively easy to talk the users down if they experience frightening sensations. In some cases, psychedelic “trips” are accompanied by music as a control aid, in the hopes of avoiding panic in the face of possible hallucinations and weird perceptions. However, physicians may nonetheless be wary of the possibility of inducing panic attacks or even psychotic episodes with their patients. It is important to screen potential subjects carefully to look for any evidence of prior susceptibility to psychotic episodes.
Despite these issues, there have been a relatively small number of randomized, controlled, though not truly double-blinded, clinical trials of both psilocybin and LSD. The studies that have been carried out more recently address a variety of disorders, with little reproduction among them in the set and setting for applying the psychedelics. This makes definitive conclusions regarding efficacy and safety of the drugs hard to come by yet. But there are some encouraging results, which we summarize below.
Figure V.2 summarizes the controlled clinical trials of psilocybin that have been completed this century, as of March 2021. The table uses data from the following sources: Carhart-Harris and Goodwin, Neuropsychopharmacology 42, 2105 (2017); Nutt, Dialogues in Clinical Neuroscience 21, 139 (2019); Mithoefer, Grob, and Brewerton, Lancet Psychiatry 3, 481 (2016); and Reiff, et al., American Journal of Psychiatry 177, 391 (2020). Note that most trials completed to date involve sample sizes of no more than about 20 subjects. The trials of treatments for cancer-driven anxiety and depression are designated in Fig. V.2 as “double-blind,” but what those studies used for placebos were often just very low doses of psilocybin, which might induce very mild hallucinogenic effects, but which still would be easily distinguishable from the larger therapeutic doses by both patients and administrators. Thus, those studies do not really meet the strict definition of a double-blind trial.

Psilocybin usage for treatment-resistant depression (TRD) has been pioneered by the Beckley Foundation/Imperial College research program led by Amanda Feilding and David Nutt. Psilocybin has by now been delivered orally to 20 patients who had been suffering from moderate to severe depression for an average of 18 years, each of whom had previously tried at least two other treatment methods without success. Each patient received two doses of psilocybin, first 10 then 25 mg, 7 days apart, accompanied by psychological support before, during and after each session. Symptoms were then periodically tested via the Quick Inventory of Depressive Symptomatology (QIDS). All showed some improvement, with maximal reduction in symptoms within 5 weeks after the larger dose (see Fig. V.3). The magnitude of the improvement was strongly correlated with the subject-reported quality of the acute psychedelic experience. Some improvement persisted even 3 months after treatment. The drug was well tolerated by all participants, and none sought conventional antidepressant treatment within 5 weeks of the second psilocybin dose.
Psychologist Alison Gopnik described the condition of these patients as one involving “an excessively narrow ego-based focus. You get stuck on the same thing, you can’t escape, you become obsessive.” She felt that exposure to psychedelics had the potential to “create an opportunity in which the old stories of who we are might be rewritten.” Gopnik used the term “brain reboot” to describe this process. Carhart-Harris prefers the more technical term of “neural plasticity.”
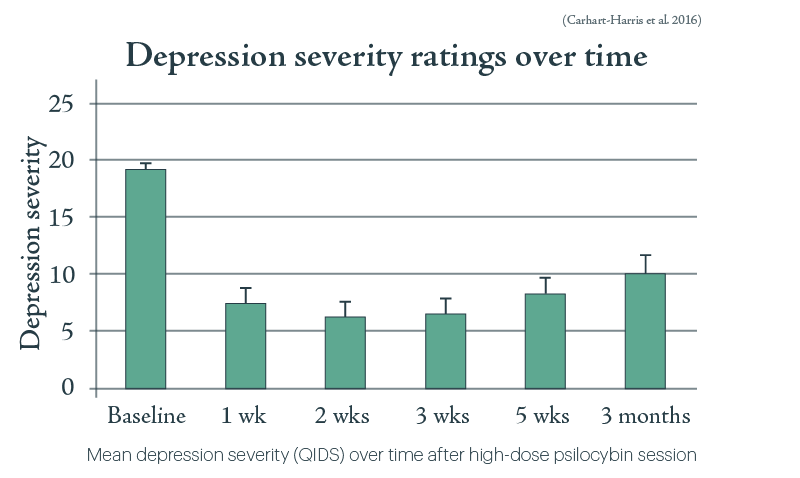
According to the Psychiatric Times article quoted earlier: “Because of these findings [in Fig. V.3] and the FDA’s designation of psilocybin as a breakthrough therapy, a phase 2b clinical trial is underway in the United States and Europe (N = 216), with additional phase 3 clinical trials planned. The phase 2b study design uses psilocybin 1 mg (considered placebo), 10 mg, and 25 mg, and the Montgomery-Asberg Depression Ratings Scales (MADRS) scores are considered the primary outcome.”
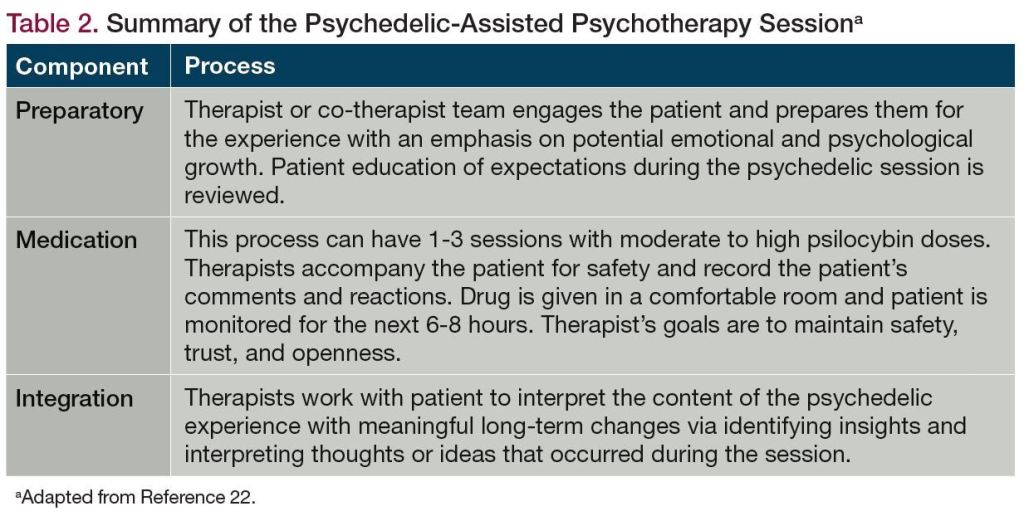
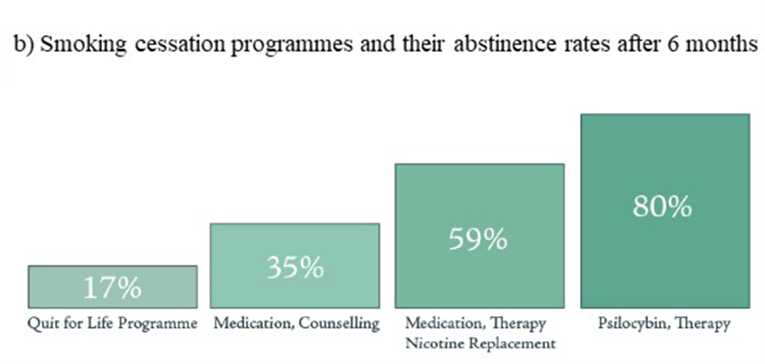
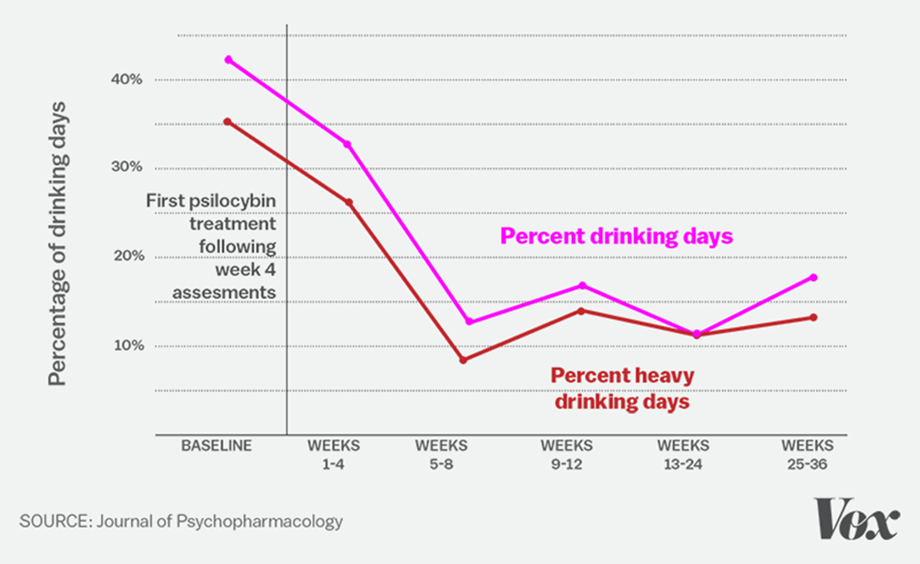
Very small studies have also provided encouraging signs that psychedelic-assisted psychotherapy may be effective in treating tobacco or alcohol dependence. The psychotherapy that accompanies these treatment protocols is summarized in Fig. V.4. As indicated, respectively, in Figs. V.5 and V.6, reduction in cigarette and alcohol use seems to persist for relatively long periods and to be achieved at greater rates than with other treatments. It is believed that the psychotherapy accompanying the drug administration is a critical feature for long-term maintenance of improvements produced by the treatment. In particular, the therapist-led discussions post drug delivery help patients to assess the psychedelic experience and what it may have taught the patients about their unhealthy brain “ruts.” Those discussions are intended to promote neural plasticity in “retraining” brain networks. However, it is important again to stress the small sample sizes and absence to date of definitive results. Larger sample controlled clinical studies will be needed.
In addition to the above studies, encouraging psilocybin results are leading to phase 2 clinical trials for treating obsessive-compulsive disorder, as well as depression, anxiety and mood disorders associated with cancer or other end-of-life conditions. Patients who experience a ‘loss of sense of self’ during the psilocybin treatment may come to see themselves as deeply connected to their environment. This may make them less fearful of dying, as they may come to see death as simply a transition to another type of existence. It is not uncommon for individuals on psychedelic drugs to “experience” both their birth and their death. This may instill in them a reassuring sense that something exists on the other side of death. Indeed, Aldous Huxley (the author of Brave New World), who was one of the first people in modern times to ingest psychedelic drugs and write about them, was an advocate of administering psychedelics to patients that were dying; he maintained that it would “make death more spiritual, and less psychological.” In fact, in 1963 as he was dying, Huxley requested that his wife inject him with LSD; she complied with his wish.
An experiment by Grob, et al. with patients suffering from advanced-stage cancer showed that administering a single moderate dose of psilocybin “significantly reduced anxiety and depression scores for months after the acute experience.” In Dec. 2016, the New York Times published an article reviewing the results of clinical trials by researchers from New York University and Johns Hopkins University that administered psilocybin to 80 patients with advanced-stage cancer. Some “80% of those patients showed clinically significant reductions in standard measures of anxiety and depression, an effect that endured for at least six months after their psilocybin session.”
Since LSD is considerably more potent than psilocybin, and more closely associated with the 1960s era of Timothy Leary’s “Turn on. Tune in. Drop out.” advice, it has been even more challenging to find funding and support for serious clinical trials since 1970. A recent systematic review of LSD therapeutic studies identified only 11 total studies that satisfied the authors’ criteria for reliable randomized and controlled clinical trials. These studies cumulatively treated 567 carefully screened patients for a variety of psychological disorders and under a variety of dosing (anywhere from 20 to 800 micrograms of LSD) and conditions, again making definitive interpretations challenging. Furthermore, a number of these trials, especially for LSD-assisted therapy of alcohol dependence, occurred before or around 1970, with somewhat mixed results regarding improved behavior of patients receiving LSD with respect to those receiving placebos with ordinary psychotherapy. In addition, one of the older trials for patients with heroin addiction even saw the LSD treatment induce “a case of prolonged psychosis…in a 21-year old patient with a previous history of recurrent psychotic episodes in the context of hospitalization during adolescence.”
Although the review authors describe results from each of these 11 trials in some detail, they come mainly to a qualitative conclusion: “Despite the design heterogeneity of clinical trials, positive results were observed, thus revealing the therapeutic potential of LSD to reduce psychiatric symptomatology, mainly in alcoholism…Despite the difficulty of designing proper double blind clinical trials with this substance, new studies that conform to modern standards are necessary in order to strengthen our knowledge on its use and open new doors in the future.”
One of the modern LSD trials included among the above 11 has since advanced to a Phase 2 clinical trial, carried out recently in Basel, Switzerland, of LSD-assisted psychotherapy for the treatment of anxiety. The trial produced clear positive results but also illustrated the challenge in trying to design a double-blind trial with psychedelics. 42 participants suffering from acute anxiety, half of them with a life-threatening illness such as cancer, were divided into two groups. At first, one of the groups received two doses of LSD while the other received two doses of a non-psychedelic placebo. But then, in a so-called “double-blind crossover” study, the two groups returned after a 24-week study period and their treatments were reversed. This crossover design was chosen “to make sure that everyone in the trial had a chance to access the LSD-assisted psychotherapy.” The patients who had received LSD in their initial treatments had significantly greater reductions in their anxiety than those who initially received the placebo, as measured with the State-Trait Anxiety Inventory (STAI), and these improvements persisted out to the last measurement 16 weeks after their second LSD dose. In fact, the improvements lasted long enough to compromise analysis of the crossover second treatment, since by then the initial LSD recipients were starting from a much better place than the initial placebo recipients, who did not show the same degree of improvement as the participants in the first group.
Advocating for rescheduling of psilocybin and LSD:
The type of large-sample phase 3 clinical trials needed to seek approval for therapeutic uses of psilocybin and LSD will be very difficult to accomplish without removal of the psychedelic drugs from Schedule I designation. In fact, psilocybin is reported to have a low abuse potential and to yield no physical dependence, based on the 8 factors included in the U.S. Controlled Substances Act. Clearly from the above pilot studies, it has potential medical uses. Thus, Johnson, et al., have recommended that psilocybin be rescheduled in the U.S. as a Controlled Substance Schedule IV drug with a Risk Evaluation and Mitigation Strategy (REMS), if approved by the U.S. Food and Drug Administration (FDA). Schedule IV drugs, such as Xanax, Valium, and Ambien, are ones judged to have low potential for abuse and low risk of dependence. According to the FDA website, REMS “is a drug safety program that the U.S. Food and Drug Administration (FDA) can require for certain medications with serious safety concerns to help ensure the benefits of the medication outweigh its risks. REMS are designed to reinforce medication use behaviors and actions that support the safe use of that medication.”
Johnson, et al., summarize the possible adverse effects of psilocybin this way (see also the discussion in Section II of this post): “Potential harms include dangerous behavior in unprepared, unsupervised users, and exacerbation of mental illness in those with or predisposed to psychotic disorders. However, scope of use and associated harms are low compared to prototypical abused drugs, and the medical model addresses these concerns with dose control, patient screening, preparation and follow-up, and session supervision in a medical facility.” There are no indications that either psilocybin or LSD is addictive. And a review of studies exploring potential long-term effects of psychedelic drugs concludes: “Our systematic review of the current psychedelic literature revealed that psychedelic experiences can lead to myriad long-lasting psychological changes and research into these effects is a growing area of study…Mystical experiences, connectedness, emotional breakthrough, and increased neural entropy were among the most commonly theorized mechanisms leading to long-term change. Psychedelics have been shown to be relatively safe when used with the proper preparation, supervision, and integration, but it is unclear the extent to which this generalizes to recreational use.”
One of the primary voices pushing for a relaxation of government-imposed restrictions on psychedelic use for medicine is Amanda Feilding, the founder of the Beckley Foundation that has funded most of the psychedelic research emerging from the U.K. She currently co-leads the Beckley/Imperial Psychedelic Research Programme with David Nutt (see Fig. V.7) and has been one of the most visionary voices in pushing for rigorous scientific evidence about the drugs. Feilding has urged the UK Prime Minister and Minister of Health to move psilocybin to Schedule II of the 1971 Misuse of Drugs Act: “Reclassifying psilocybin as a Schedule II drug would greatly increase access for researchers and enable doctors to prescribe to those in need without any change to legislation governing recreational use, and as such should be considered solely on its significant scientific and medical merit.” According to Feilding, the bureaucratic and financial obstacles imposed by Schedule I classification currently make research on psychedelics cost five to ten times as much as research on Schedule II drugs.
Even if the drugs are rescheduled, physicians may be reluctant to provide psychedelic drugs to their patients. First, the business model for psychiatrists is one where their patients make regular visits, often for extended periods of time. The role of the “guide” in administering psychedelics is terribly important (this is an essential part of the “set and setting” in administering the drug); however, with psychedelic drugs the role of the guide is intermediate between the traditional role of the physician and that of a mystic or shaman, and psychiatrists may shy away from that role.
Nevertheless, a group of European physicians are convinced that they can build clinics where patients would come for treatment with psilocybin or LSD. The patients would be treated by “board certified” practitioners in psychedelic medicine. The entrepreneurs have raised several million Euros to fund clinical trials for medical applications of psilocybin. They believe that psychedelic treatment centers could flourish in the same way that fitness centers, yoga and massage clinics have mushroomed (so to speak).
It is even possible that treatment with psychedelics will flourish abroad, but fall victim to politics in the U.S. A recent Attorney General, Jeffrey Beauregard Sessions, was eager to re-ignite the War on Drugs. Sessions stated that marijuana use was a “life-wrecking dependency” that was “only slightly less awful” than heroin. Note that from 1999 – 2000 143,000 Americans died from heroin overdoses; approximately zero died from direct effects of marijuana. In May 2017 Sessions ordered federal prosecutors to seek the maximum criminal charges in drug cases. In March 2018 he instructed federal prosecutors to seek the death penalty for major drug dealers. Almost all Congressional Republicans oppose making possession of cannabis legal, despite the fact that 37 states (plus the District of Columbia, Guam, Puerto Rico and the U.S. Virgin Islands) have legalized possession of pot. So it is conceivable that research into the effects of psychedelic substances on the brain, and the potential for medical applications of drugs such as psilocybin, may never materialize in the U.S., even if such drugs become widely used and widely effective abroad. In other words, there may be an American political group that is only too willing to extend our disastrous War on Drugs into the foreseeable future. This may prove once again philosopher George Santayana’s adage that “Those who cannot remember the past are condemned to repeat it.”
VI. summary and outlook
Neuroimaging studies of subjects given moderate doses of psilocybin or LSD have been pioneered during this century by groups centered at Imperial College London and the University of Zurich. These studies have already revealed the radical changes in brain activity and neural connections which these psychedelic drugs induce by strongly activating so-called 5-HT2A serotonin receptors densely distributed throughout the cerebral cortex in human brains. The Default Mode Network that normally dominates the self-reflective state of the brain is suppressed, while unusual connections are activated among different brain regions. These changes lead to a “hyperconnectedness” that explains many of the qualitative features self-reported by users of the psychedelic drugs: hallucinations, mixed-up sensory perceptions, a loss of boundaries between the self and the external world, and an expansion of consciousness.
These profound alterations in brain function can be frightening in unsupervised users and resulting “bad trips” led to both psychedelic drugs being classified by 1970 as Schedule I drugs with high potential for abuse and no known medical applications. However, it was also realized that in a supervised and controlled setting these brain alterations might have therapeutic applications in treating a variety of mental disorders. The entropic brain model proposed by Robin Carhart-Harris and collaborators to encompass both their neuroimaging results and a variety of mental disorders helps to clarify where psychedelics may be useful in therapy. In their model, the psychedelics induce a sharp increase in entropy within the brain of a patient, and therefore may have benefit for those suffering from disorders characterized by inflexible mental processes of low entropy: e.g., depression, anxiety, obsessive-compulsive disorder, and various addictions. On the other hand, psychedelic treatments should be avoided for those already susceptible to high-entropy mental disorders such as schizophrenia or other psychoses characterized by formless mental processes poorly constrained by reality. Without careful supervision and preparation, application of psychedelics can possibly trigger psychotic episodes.
The increased 21st-century understanding of the neurochemical basis for psychedelic effects has stimulated a number of recent clinical studies to assess the drugs’ efficacy and dangers in assisting psychotherapy. These clinical studies are still at an early stage and involve relatively small numbers of subjects. The studies are challenged in a number of ways: by the absence of funding from either governments or large pharmaceutical companies; by the difficulty in designing “double-blind” trials where neither subjects nor administrators know who has received the psychedelic drugs and who the placebo; by the need for careful pre-screening of the psychiatric history of participants and calming oversight, preferably by a psychiatrist, of each patient before, during, and after administration of the psychedelics; and by the absence of general agreement on the preferred set and setting of the drug delivery.
Despite these challenges the clinical studies have already produced encouraging results. Psilocybin-assisted psychotherapy has produced clear improvements in patients suffering from treatment-resistant depression, dependences on tobacco or alcohol, obsessive-compulsive disorder, and severe anxiety driven by life-threatening illnesses such as cancer. LSD-assisted psychotherapy has also shown promise for treating alcoholism and anxiety. The improvements furthermore have some staying power; they seem to persist at least months after the drug sessions. The results have led, for example, to the U.S. Food and Drug Administration’s 2018 designation of psilocybin-assisted psychotherapy as a “breakthrough therapy” for treatment-resistant depression. And a few Phase 2 clinical trials are now completed or under way.
The FDA designation, however, still falls far short of full drug approval. Before psychedelic therapies can be authorized generally, a great deal of additional research and far more extensive clinical trials are necessary, along with government action to reschedule the drug classifications. Funding must be sought for randomized and placebo-controlled Phase 3 clinical trials with large numbers of participants and careful selection of control groups that match those who will receive the drugs as closely as possible, to minimize confounding variables. Trials carried out in different locations by different supervising groups will have to be shown to produce reproducible results. Participants will have to be monitored periodically over longer time periods to look for possible long-term side-effects of the drugs and to judge the permanence of the improvements. Results obtained with psilocybin can be compared to those obtained with LSD to judge whether one of these classic psychedelics is preferred over the other. Neuroimaging of patients who do show lasting improvement, both before and at various intervals after treatment, will be useful to assess whether there are indeed permanent changes in the functional connectivity of different brain regions, changes that might be attributed to neural plasticity. Further neuroimaging experiments can also help to test and quantify the entropic brain model.
The disorders which psychedelic-assisted psychotherapy can potentially treat are debilitating. They account for substantial losses in productivity in industrialized countries and their treatment represents a significant fraction of health care costs. But even if future Phase 3 trials demonstrate that psilocybin and LSD provide greater efficacy and efficiency, along with less severe side-effects, than other approaches in treating these disorders, one will still need to overcome the serious stigma these psychedelic drugs carry in social perceptions and political wrangling, before such treatments can gain widespread approval.
References:
Michael Pollan, How to Change Your Mind: What the New Science of Psychedelics Teaches Us About Consciousness, Dying, Addiction, Depression and Transcendence (Penguin Press, 2018), https://michaelpollan.com/books/how-to-change-your-mind/
Robin Carhart-Harris, Brain Imaging Studies with Psilocybin and MDMA, talk at Psychedelic Science 2013 Conference, https://www.youtube.com/watch?v=CNR4o5JZEi0
Robin Carhart-Harris, Psychedelics, keynote speech at The Science of Consciousness 2022 Conference, https://www.youtube.com/watch?v=Ac2Iq3ZLI5E
Centre for Psychedelic Research, Imperial College London, https://www.imperial.ac.uk/psychedelic-research-centre/
https://www.beckleyfoundation.org/
https://en.wikipedia.org/wiki/Amanda_Feilding
F.X. Vollenweider, Neurophenomenology of Consciousness, University of Zurich research group, https://www.dppp.uzh.ch/en/researchgroups/researchgroups/neurophenomenology-of-consciousness.html
Psychedelics Division, University of California at San Francisco, https://neuroscape.ucsf.edu/psychedelics/
Drug Scheduling, U.S. Drug Enforcement Agency, https://www.dea.gov/drug-information/drug-scheduling
Y. Saplakoglu, FDA Calls Psychedelic Psilocybin a ‘Breakthrough Therapy’ for Severe Depression, LiveScience, Nov. 25, 2019, https://www.livescience.com/psilocybin-depression-breakthrough-therapy.html
The Psychedelic Renaissance and the Importance of Drug Policy Reform, Open Access Government, Dec. 12, 2019, https://www.openaccessgovernment.org/drug-policy-reform/79314/
Wikipedia, Psilocybin, https://en.wikipedia.org/wiki/Psilocybin
Wikipedia, Florentine Codex, https://en.wikipedia.org/wiki/Florentine_Codex
R. Gordon Wasson, Seeking the Magic Mushroom, Life magazine, May 13, 1957, https://www.biblio.com/book/life-magazine-may-13-1957-seeking/d/1296080826
Wikipedia, Albert Hoffman, https://en.wikipedia.org/wiki/Albert_Hofmann
Wikipedia, Timothy Leary, https://en.wikipedia.org/wiki/Timothy_Leary
Wikipedia, Harvard Psilocybin Project, https://en.wikipedia.org/wiki/Harvard_Psilocybin_Project
Wikipedia, Concord Prison Experiment, https://en.wikipedia.org/wiki/Concord_Prison_Experiment
Wikipedia, Marsh Chapel Experiment, https://en.wikipedia.org/wiki/Marsh_Chapel_Experiment
Wikipedia, Rick Doblin, https://en.wikipedia.org/wiki/Rick_Doblin
Controlled Substances Act, U.S. Drug Enforcement Agency, https://www.dea.gov/drug-information/csa
Psilocybin (magic mushrooms), Australian Alcohol and Drug Foundation, https://adf.org.au/drug-facts/psilocybin/
D. Lattin, The Harvard Psychedelic Club (Harper Collins, 2010), https://www.amazon.com/Harvard-Psychedelic-Club-Timothy-Fifties/dp/0061655945
R.S. Gable, “Acute toxicity of drugs versus regulatory status“, In J.M. Fish, Drugs and Society: U.S. Public Policy. Lanham, Maryland (Rowman & Littlefield. 2006), p. 149, https://web.cgu.edu/faculty/gabler/drug_toxicity.htm
What is the Most Dangerous Drug?, The Economist, June 2019 https://www.economist.com/graphic-detail/2019/06/25/what-is-the-most-dangerous-drug 25
D.J. Nutt, L.A. King, and L.D. Phillips, Drug Harms in the UK: A Multicriteria Decision Analysis, The Lancet 376, 1558 (2010), https://www.thelancet.com/action/showPdf?pii=S0140-6736%2810%2961462-6
L. Wright, Rat Studies Elucidate the Neurochemistry of Addiction, Scientific American, April 10, 2003, https://www.scientificamerican.com/article/rat-studies-elucidate-the/
Aldous Huxley, The Doors of Perception (Harper & Row, 1954), https://en.wikipedia.org/wiki/The_Doors_of_Perception
William Blake, The Marriage of Heaven and Hell, 1794, https://www.gutenberg.org/files/45315/45315-h/45315-h.htm
Wikipedia, Lysergic Acid Diethylamide, https://en.wikipedia.org/wiki/Lysergic_acid_diethylamide
Richard Condon, The Manchurian Candidate (McGraw-Hill 1959), https://en.wikipedia.org/wiki/The_Manchurian_Candidate
The Manchurian Candidate, 1962 movie directed by John Frankenheimer, released by United Artists, https://en.wikipedia.org/wiki/The_Manchurian_Candidate_(1962_film)
Wikipedia, MKUltra, https://en.wikipedia.org/wiki/MKUltra
Wikipedia, Nuremberg Code, https://en.wikipedia.org/wiki/Nuremberg_Code
Stephen Kinzer, Poisoner in Chief: Sidney Gottlieb and the CIA Search for Mind Control (Henry Holt & Co., 2019), https://www.amazon.com/Poisoner-Chief-Sidney-Gottlieb-Control/dp/1250140439
Wikipedia, Abu Ghraib Torture and Prisoner Abuse, https://en.wikipedia.org/wiki/Abu_Ghraib_torture_and_prisoner_abuse
S. Weinberger, When the CIA Was Into Mind Control, New York Times, Sept. 10, 2019, https://www.nytimes.com/2019/09/10/books/review/poisoner-in-chief-stephen-kinzer.html
S.M. Hersh, Huge CIA Operation Reported in U.S. Against Anti-war Forces, Other Dissidents in Nixon Years, New York Times, Dec. 22, 1974, https://www.nytimes.com/1974/12/22/archives/huge-cia-operation-reported-in-u-s-against-antiwar-forces-other.html
Wikipedia, Church Committee, https://en.wikipedia.org/wiki/Church_Committee
WIkipedia, United States President’s Commission on CIA Activities Within the United States, https://en.wikipedia.org/wiki/United_States_President%27s_Commission_on_CIA_Activities_within_the_United_States
Timothy Leary, High Priest (Ronin Press 1968), https://www.amazon.com/High-Priest-Leary-Timothy/dp/0914171801
Wikipedia, Ken Kesey, https://en.wikipedia.org/wiki/Ken_Kesey
Wikipedia, The Merry Pranksters, https://en.wikipedia.org/wiki/Merry_Pranksters
Wikipedia, The Electric Kool-Aid Acid Test, https://en.wikipedia.org/wiki/The_Electric_Kool-Aid_Acid_Test
Wikipedia, Love Pageant Rally, https://en.wikipedia.org/wiki/Love_Pageant_Rally
Wikipedia, Human Be-In, https://en.wikipedia.org/wiki/Human_Be-In
Wikipedia, Art Linkletter, https://en.wikipedia.org/wiki/Art_Linkletter
DebunkingDenial, Reefer Madness: The U.S. War on Cannabis, https://debunkingdenial.com/reefer-madness-the-u-s-war-on-cannabis/
DebunkingDenial, My Brain Surgery, https://debunkingdenial.com/my-brain-surgery/
DebunkingDenial, Brainwashing via Social Media, https://debunkingdenial.com/brainwashing-via-social-media/
R.P.N. Rao and D.H. Ballard, Predictive Coding in the Visual Cortex: A Functional Interpretation of Some Extra-Classical Receptive Field Effects, Nature Neuroscience 2, 79 (1999), https://www.nature.com/articles/nn0199_79
The Neuroscience of Psychedelics: This is Your Brain on Drugs (Literally), https://www.inverse.com/mind-body/what-happens-in-your-brain-when-you-hallucinate
C.J. Harmer and M. Browning, Can a Predictive Processing Framework Improve the Specification of Negative Bias in Depression?, Biological Psychiatry 87, 382 (2020), https://pubmed.ncbi.nlm.nih.gov/32029072/
M.H. Herzog and A.M. Clarke, Why Vision is Not Both Hierarchical and Feed-Forward, Frontiers in Computational Neuroscience 8, 135 (2014), https://www.frontiersin.org/articles/10.3389/fncom.2014.00135/full
R.L. Carhart-Harris and K.J. Friston, REBUS and the Anarchic Brain: Toward a Unified Model of the Brain Action of Psychedelics, Pharmacological Reviews 71, 316 (2019), https://pharmrev.aspetjournals.org/content/71/3/316
Serotonin, Cleveland Clinic, https://my.clevelandclinic.org/health/articles/22572-serotonin
Wikipedia, Serotonin, https://en.wikipedia.org/wiki/Serotonin
Wikipedia, Psilocin, https://en.wikipedia.org/wiki/Psilocin
N. Banerjee, Neurotransmitters in Alcoholism: A Review of Neurobiological and Genetic Studies, Indian Journal of Human Genetics 20, 20 (2014), https://www.researchgate.net/publication/262675156_Neurotransmitters_in_alcoholism_A_review_of_neurobiological_and_genetic_studies/link/0a85e53861e09a7388000000
Wikipedia, Ketanserin, https://en.wikipedia.org/wiki/Ketanserin
K.H. Preller, et al., Effective Connectivity Changes in LSD-Induced Altered States of Consciousness in Humans, Proceedings of the National Academies of Sciences (PNAS) 116, 2743 (2019), https://www.pnas.org/doi/10.1073/pnas.1815129116
Wikipedia, Default Mode Network, https://en.wikipedia.org/wiki/Default_mode_network
M.E. Raichle, et al., A Default Mode of Brain Function, Proceedings of the National Academies of Sciences (PNAS) 98, 676 (2001), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC14647/
A. Horn, D. Ostwald, M. Reisert, and F. Blankenburg, The Structural-Functional Connectome and the Default Mode Network of the Human Brain, NeuroImage 102, 142 (2014), https://www.sciencedirect.com/science/article/abs/pii/S1053811913010057?via%3Dihub
R. Carhart-Harris, et al., Neural Correlates of the Psychedelic State as Determined by fMRI Studies with Psilocybin, Proceedings of the National Academies of Sciences (PNAS) 109, 2138 (2012). https://www.pnas.org/doi/10.1073/pnas.1119598109
H. Lv, et al., Resting-State Functional MRI: Everything That Nonexperts Have Always Wanted to Know, American Journal of Neuroradiology (Jan. 2018), http://www.ajnr.org/content/early/2018/01/18/ajnr.A5527
R. Carhart-Harris, et al., Psilocybin With Psychological Support for Treatment-Resistant Depression, Lancet Psychiatry 3, 619 (2016), https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(16)30065-7/fulltext
R. Carhart-Harris, et al., How do Hallucinogens Work on the Brain?, Psychologist 27, 663 (2014), https://www.bps.org.uk/psychologist/how-do-hallucinogens-work-brain
R. Carhart-Harris, et al., The Entropic Brain: a Theory of Conscious States Informed by Neuroimaging Research With Psychedelic Drugs, Frontiers in Human Neuroscience 8, 20 (2014), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3909994/pdf/fnhum-08-00020.pdf
Z. Cormier, Brain Scans Reveal How LSD Affects Consciousness, Nature 2016, 19727, https://www.nature.com/articles/nature.2016.19727
R.L. Carhart-Harris, et al., Neural Correlates of the LSD Experience Revealed by Multimodal Neuroimaging, Proceedings of the National Academies of Sciences (PNAS) 113, 4853 (2016), https://www.pnas.org/doi/full/10.1073/pnas.1518377113
G. Petri, et al., Homological Scaffolds of Brain Functional Networks, Journal of the Royal Society Interface 11, 20140873, https://royalsocietypublishing.org/doi/pdf/10.1098/rsif.2014.0873
M.M. Nour, et al., Psychedelics, Personality and Political Perspectives, Journal of Psychoactive Drugs 1 (2017), https://www.tandfonline.com/doi/full/10.1080/02791072.2017.1312643
M.W. Jann, Psilocybin Revisited: The Science Behind the Drug and Its Surprising Therapeutic Potential, Psychiatric Times 38, March 10, 2021, https://www.psychiatrictimes.com/view/psilocybin-revisited-science-behind-drug-surprising-therapeutic-potential
R.L. Carhart-Harris and G.M. Goodwin, The Therapeutic Potential of Psychedelic Drugs: Past, Present, and Future, Neuropsychopharmacology 42, 2105 (2017), https://www.nature.com/articles/npp201784
M.C. Mithoefer, C.S. Grob, and T.D. Brewerton, Novel Psychopharmacological Therapies for Psychiatric Disorders: Psilocybin and MDMA, Lancet Psychiatry, May 2016, 481, https://pubmed.ncbi.nlm.nih.gov/27067625/
C.M. Reiff, et al., Psychedelics and Psychedelic-Assisted Psychotherapy, American Journal of Psychiatry 177, 391 (2020), https://pubmed.ncbi.nlm.nih.gov/32098487/
M. Rupp, The Psychedelic Experience, https://sapiensoup.com/psychedelic-experience
The Beckley/Imperial Psychedelic Research Programme, https://www.beckleyfoundation.org/science/collaborations/the-beckley-imperial-psychedelic-research-programme/
A. Yeung, et al., The Quick Inventory of Depressive Symptomatology, Clinician Rated and Self-Report, Journal of Nervous and Mental Disorders Aug. 2012, 712, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3762496/
Wikipedia, Montgomery-Asberg Depression Rating Scale, https://en.wikipedia.org/wiki/Montgomery%E2%80%93%C3%85sberg_Depression_Rating_Scale
M.W. Johnson, A. Garcia-Romeu, and R.R. Griffiths, Long-term Follow-up of Psilocybin-Facilitated Smoking Cessation, American Journal of Drug and Alcohol Abuse 43, 55 (2017), https://pubmed.ncbi.nlm.nih.gov/27441452/
M.P. Bogenschutz, et al., Psilocybin-Assisted Treatment for Alcohol Dependence: A Proof-of-Concept Study, Journal of Psychopharmacology 29, 289 (2015), https://pubmed.ncbi.nlm.nih.gov/25586396/
C.S. Grob, et al., Pilot Study of Psilocybin Treatment for Anxiety in Patients With Advanced-Stage Cancer, Archives of General Psychiatry 68, 71 (2011), https://jamanetwork.com/journals/jamapsychiatry/fullarticle/210962
J. Hoffman, A Dose of a Hallucinogen from a ‘Magic Mushroom,’ and Then Lasting Peace, New York Times, Dec. 1, 2016, https://www.nytimes.com/2016/12/01/health/hallucinogenic-mushrooms-psilocybin-cancer-anxiety-depression.html
J.J. Fuentes, et al., Therapeutic Use of LSD in Psychiatry: A Systematic Review of Randomized-Controlled Clinical Trials, Frontiers in Psychiatry, Jan. 21, 2020, https://www.frontiersin.org/articles/10.3389/fpsyt.2019.00943/full
Wikipedia, Aldous Huxley, https://en.wikipedia.org/wiki/Aldous_Huxley
C. Savage and O.L. McCabe, Residential Psychedelic (LSD) Therapy for the Narcotic Addict: A Controlled Study, JAMA Psychiatry 28, 808 (1973), https://jamanetwork.com/journals/jamapsychiatry/article-abstract/490914
P. Gasser, K. Kirchner, and T. Passie, LSD-Assisted Psychotherapy for Anxiety Associated with a Life-Threatening Disease: A Qualitative Study of Acute and Sustained Subjective Effects, Journal of Psychopharmacology 29, Issue 1 (2014), https://journals.sagepub.com/doi/abs/10.1177/0269881114555249
R.J. Mackenzie, LSD for Anxiety: A Deep Dive into a New Clinical Trial, Neuroscience News and Research, Oct. 7, 2022, https://www.technologynetworks.com/neuroscience/articles/lsd-for-anxiety-a-deep-dive-into-a-new-clinical-trial-366381
Crossover Study, https://www.winchesterhospital.org/health-library/article?id=41429
Wikipedia, State-Trait Anxiety Inventory, https://en.wikipedia.org/wiki/State-Trait_Anxiety_Inventory
Why Rescheduling LSD and Psilocybin Would Transform Research into Treating Depression and Anxiety, Beckley Foundation, https://www.beckleyfoundation.org/2017/10/12/the-case-for-rescheduling-psychedelics/
M.W. Johnson, et al., The Abuse Potential of Medical Psilocybin According to the 8 Factors of the Controlled Substances Act, Neuropharmacology 142, 143 (2018), https://www.sciencedirect.com/science/article/pii/S0028390818302296
Risk Evaluation and Mitigation Strategies/REMS, U.S. Food and Drug Administration, https://www.fda.gov/drugs/drug-safety-and-availability/risk-evaluation-and-mitigation-strategies-rems
J.S. Aday, et al., Long-Term Effects of Psychedelic Drugs: A Systematic Review, Neuroscience and Biobehavioral Reviews 113, 179 (2020), https://www.sciencedirect.com/science/article/abs/pii/S0149763419310413?via%3Dihub
J. Richardson, Jeff Sessions Thinks Pot is as Bad as Heroin. That’s So Wrong, Mar. 22, 2017, https://otherwords.org/jeff-sessions-thins-pot-is-as-bad-as-heroin-thats-so-wrong/
Wikipedia, Jeff Sessions, https://en.wikipedia.org/wiki/Jeff_Sessions
Drug Overdose Deaths, Centers for Disease Control Injury Center, https://www.cdc.gov/drugoverdose/deaths/heroin/index.html
George Santayana, The Life of Reason, 1905 (from the series Great Ideas of Western Man), https://americanart.si.edu/artwork/those-who-cannot-remember-past-are-condemned-repeat-it-george-santayana-life-reason-1905
