
Steve Vigdor, June 29, 2021
I. Introduction
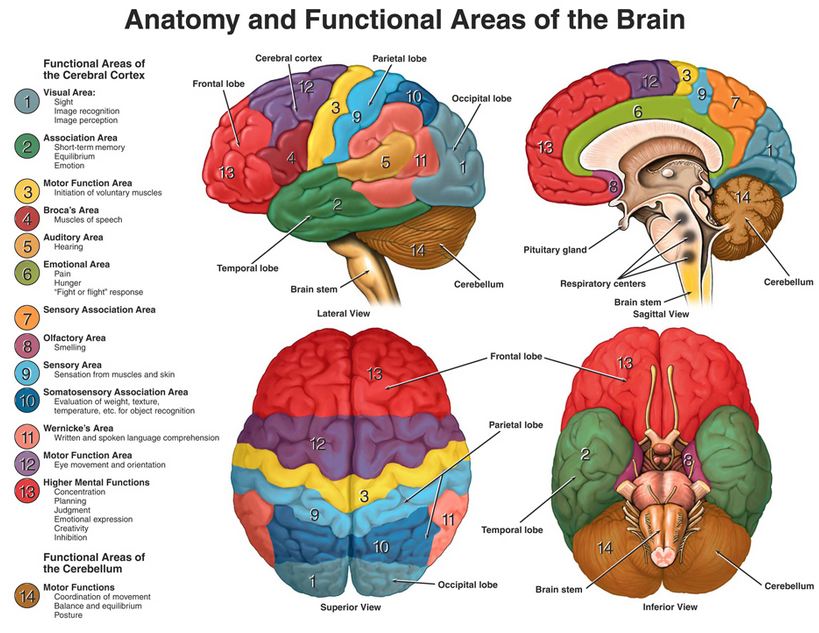
The human brain is a compact, intricate marvel. It governs such involuntary bodily functions as breathing, all of our sensory perceptions of and reactions to the outside world, our motor functions, speech, hearing and understanding of language, thoughts, memories, ideas, emotions, creativity, and judgments. It self-regulates body temperature, blood pressure, heart rate, fluid and hormonal balances to maintain system equilibrium, or homeostasis, and the circadian rhythm that allows us to be active during daylight hours and sleep at night. It does all this by a division of labor among parts of the brain’s anatomy that is only hinted at in Figs. 1 and 2, of the outer cerebral cortex and inner limbic systems, respectively. In a healthy brain all of these parts work in concert, receiving and sending signals via billions of neurons to all body parts and organs, allowing an individual to function productively and responsively in his/her environment.

I have always considered my own brain function to be healthy, facilitating clear-eyed perceptions, rational thinking and judgments, awareness of my emotional state and calm, creative problem-solving in stressful situations. But very recently I experienced a rapid onset of deviations from my normal brain functioning, which led in short order to hospitalization and neurosurgery. I am not a neuroscientist, but I am a scientist, and have therefore been very curious to understand – with the aid of numerous physicians and articles – just what went wrong. This blog post relays my personal story and evolving understanding; it thus differs from our usual posts debunking aspects of science denial. Given its functional complexity, there are numerous ways our brains can adversely affect our health. By way of foreshadowing, my own problems centered on the tiniest subsystem in Fig. 1, the pea-sized pituitary gland lying just above the brain stem.
II. The symptoms
My symptoms began in early May 2021 in Arizona. My wife and I, having both received two COVID vaccine doses by early March, were there on our first vacation in well over a year. We started out for a few days in Phoenix, but then drove up to witness sunset (Fig. 3) and sunrise (Fig. 4) over the Grand Canyon. We hiked part way down, and then back up, the Bright Angel trail (Fig. 5) into the Canyon. We then drove down to Sedona, where we hiked up a narrow trail in the mountains just outside Sedona (Fig. 6) on the morning of May 5. On the morning of May 6, in Scottsdale, I awoke after a night of fitful sleep with a tension headache and a feeling of grogginess. Nonetheless, we went about our planned activities, swimming and visiting local sites. The headache and grogginess persisted on the 7th, but still did not limit our plans. We attributed my symptoms to a possible response to the 100°F heat. This concludes the travelog section of this post.




The first sign of something quite peculiar about my vision came at the Phoenix airport on May 8, as we prepared for our flight back home to Indiana. I managed to drop my new smart phone on the floor at the security check-in and reported to my wife that afterwards the phone was no longer responding reasonably, in the sense that the letters came out mostly wrong when I attempted to send text messages. However, she tried my phone and found nothing amiss. I later determined, in the hospital but before my surgery, that if I clicked slightly to the left of the positions where my brain “saw” the letters on my phone, it worked fine for me as well. When I drove us home from the Indianapolis airport to Bloomington late that evening, my wife commented that I was veering out of my lane much more than was characteristic. But she attributed this to my tiredness after a long day.
On May 9 I developed chills and a substantial fever, accompanying the persistent headache and grogginess. On May 10 all of the symptoms remained, but the grogginess graduated into dizziness. I determined that it was important to visit my primary care physician to figure out what was going on, but I would not be allowed into the care facility without a negative COVID test, given my fever. So my wife scheduled a test for me that afternoon at the town’s free testing site, for 2:45 pm, just before the facility would close for the day at 3:00 pm. She gave me the address of the testing site and told me to just drive north on Morton Street until I saw it. However, I misunderstood that the testing site was operated by the county, and not by IU Health, the dominant organization of physicians and hospitals in the state of Indiana. I therefore stopped first on Morton Street when I saw an IU Health facility.
The people working inside informed me that I was at the wrong place, but just had to drive a short distance further north on Morton, and then I “couldn’t miss” the testing site. On trying to leave the IU Health facility, I was unable to start my car. After I had tried in vain for about 20 minutes, one of the IU Health workers came out to show me that my foot was not, as I thought, on the brake pedal, but was displaced to one side. After helping me correct this rather absurd failure, the worker repeated the directions to find the testing site. Note to future samaritans: giving directions to a driver who has just been unable to locate his brake pedal may seem helpful, but is not a good idea.
I drove further north as instructed, but failed to see a site I was told I couldn’t miss. So I continued to drive north, even though this required my crossing an island on one cross-street and then driving through barriers that were clearly intended to limit further passage to bikes and pedestrians. However, I judged that the posts in that barrier were just far enough apart that my car could squeeze through. I executed my irrational decision precisely, with the passenger-side side-view mirror folding in slightly as it brushed against the post to my right, but then springing back to its normal position, just as it was designed to do. Having concentrated on safe passage through that barrier, I was disappointed to see a clear dead end ahead, so I decided to park my car in an adjacent lot and continue on foot.
I knew I was too far north at that point, so I walked back south but still failed to find the testing site I couldn’t miss. With my stress level building, as I was hoping to find the site still open even though its official closing time had already passed, I turned back north again and eventually got dizzy and fell. I clearly was not problem-solving calmly under stress in performing what seemed to be a simple task. I would later learn that the problem was, in fact, not solvable because the testing site closed promptly at 3 pm and took in all the signage that indicated the presence of a COVID testing site. The only sign left was the word “Laundry” on the front of the building, hardly the “can’t-miss” signal I expected.
Three young ladies driving by saw me fall and one of them called an ambulance. It wasn’t a bad fall – I scraped my knee and nose and jammed a thumb – but we were only a few blocks from the IU Health Bloomington Hospital and the ambulance arrived before I got up. The emergency technician advised me not to get up and asked whether I was on alcohol or drugs. I assured him I wasn’t but then was unable to recall the name of the one prescription drug I take regularly. Noting my confusion, he and the driver put me on a stretcher and drove me straight to the Emergency Room to assess what was going on with me.
At the Emergency Room they determined quickly that I was running a significant fever, my breathing was labored, and my blood work indicated impaired kidney function. A CT scan revealed a mass nearly one inch in diameter lying within a small nook, called the Sella, containing the pituitary gland and adjacent to the optical chiasm where the optic nerves from the left and right eyes cross on their way to the brain (see Fig. 7). An MRI scan of my brain showed that the mass was impinging on the optic nerves and very likely causing vision problems. I would later be told that the mass was also impinging on the pituitary gland itself, contributing to many of my symptoms. The only good news was that the MRI revealed no other unexpected structures in my brain.

In the midst of all these tests, my wife phoned to see what had happened to me and where I had left my car, so that she could retrieve it and drive it home. I told her I parked it in a lot adjacent to Morton St. She called back some time later to say that she had finally found the car after searching for a long time, but that I couldn’t possibly have gotten to that lot from Morton St. because that entrance is inaccessible to cars. I assured her that my memory did not seem to be affected by all my ailments and irrational decision-making, and that I had, in fact, driven through barriers she assured me no car could fit between.
Doubting my memories, she said she would come later to the hospital to retrieve my car keys, since the battery in her key fob for my car had run out. I told her she had to hurry because the doctors had just informed me that the pituitary mass would have to be removed surgically, but that it required a type of skull neurosurgery for which there was no expertise in Bloomington. They were thus about to load me into another ambulance to whisk me up to IU Health Methodist Hospital in Indianapolis, which houses a neuroscience center and has several neurosurgeons with experience in removing the sort of adenoma (tumor) I seemed to have.
I arrived at Methodist Hospital toward 10 pm on May 10. The admitting doctor in the Emergency Room there told me that I would probably need another CT, and possibly MRI, scan. I replied “Oh, no! I just had an MRI in Bloomington and it was a nightmare” keeping my head perfectly still inside a small enclosure for 40 minutes of imaging accompanied by extremely loud noises, even with the plugs they had inserted in my ears. (I still don’t understand why MRI scans ever needed to be anywhere near that loud.) Fortunately, a member of the neurosurgery team entered at just that moment and assured me I wouldn’t need another MRI, though they did want a CT scan of my skull in order to plan the surgery I would need. However, he said they would not perform the surgery until they understood and managed the root cause of my diverse symptoms, which might or might not be the pituitary mass. In particular, he informed me that the sort of pituitary adenoma I seemed to have grows very slowly, and normally leads to a very gradual, rather than sudden, onset of symptoms. His approach seemed a reasonable and prudent course of action, but it led to a 15-day hospitalization.
III. the hospitalization
As my daughter put it, “How can this man, who seemed perfectly healthy only days before, and who hasn’t previously spent even a single night since birth as a hospital in-patient, suddenly have breakdowns in so many organs? There must be a common cause for all the symptoms.” For the ensuing week all sorts of doctors and nurses searched for that common cause. I was attended by members of the neurosurgery team, the pulmonology team, the endocrinology team, the infectious disease team, the gastro-intestinal team, and at the urging of my daughter based on her concerns that all my problems might signal an auto-immune disorder, the rheumatology team as well. Continuous heart monitoring revealed healthy heart rhythms, so I did manage to avoid the cardiology team. The sheer number of different doctors I saw each day led me to question who was really in charge of my case. Several times I heard from nurses attending me that my case reminded them of the TV series House, in which the antisocial Dr. House uses his wits to solve baffling medical conditions characterized by diverse and apparently unrelated symptoms. But there was no Dr. House on my case.
On my second day in the hospital, when I was still housed temporarily in the Emergency Room, the doctors had me sent over to Methodist’s Eye Clinic, where they put me through visual field tests. In these, one stares with one eye at a time at a central dot on a screen and presses a clicker each time the eye and brain perceive a brief flash of light in the periphery. The flashes occur at random times and locations, and they span a wide range in intensity from very dim to relatively bright. The results were stark, showing essentially a complete loss of peripheral vision toward opposite sides in my two eyes. I was assured by ophthalmologists that this was a typical symptom of a pituitary adenoma pressing on the optic chiasm, so the result confirmed the tumor diagnosis. The next day, looking out the window of my new room on the neurosurgery floor, I found that with both eyes open my peripheral vision was blurry to both left and right. The good news was that the tumor did not appear to affect the muscles that move one’s eyes to track visual stimuli. In addition, I was told that my peripheral vision might improve once the tumor was removed, depending on how many fibers within the optic nerves were squashed irrevocably.
After the first two nights at the hospital the nurses had enough confidence in my stability on my feet to allow me to get up from bed on my own and drag my IV with me to the bathroom. But on the third day, the long IV tube got tangled up in the bed’s siderail, leading the stand and then me to fall over. This led to another brain CT scan, shortly followed by a chest CT scan to see what was going on in my lungs. The good news was that my fall did not lead to any apparent further change in my brain. The bad news was that the chest scan did reveal some murky substance confined to the upper right lung lobe, signaling some form of pneumonia.
After my fall at the hospital, I was confined to bed and required the aid of a nurse to help me stand and walk. I was then subjected to several nasal swab tests for viruses, two or more blood draws per day to search for (abundant) evidence of infections, and a bronchoscopy for which I was anaesthetized and intubated to allow extraction of both fluid and lung tissue samples from my upper right lung. The purpose of the bronchoscopy was to determine whether I had a viral, a bacterial, or a fungal infection. I urged the doctors to check in particular for evidence in my blood samples of valley fever, a fungal infection prevalent in Arizona. The lung tissue samples could be checked for evidence of either cancerous or non-cancerous growths (called granulomas, whose presence, according to my son’s Google searching, might accompany the type of sudden symptom onset I had experienced). The next few days were marked by high fevers and periodic Tylenol doses to sweat off the fever. Based on the signs of pneumonia, they put me on a five-day treatment with antibiotics designed to handle the default case of “community” pneumonia, along with several other medications.
Lab results for a number of the blood and bronchoscopy samples took up to a week to come back. During that week I was further subjected to a couple of ultrasound scans of my kidneys and abdominal region, a chest X-ray to see if the antibiotics were having any discernible effect on my lung yet, and to many further blood tests. By the end of my first week in the hospital the antibiotic treatment seemed to eliminate my fevers. But the lab results that had come back were all negative and we were no closer to understanding what sort of infection I had and what it had, if anything, to do with my pituitary tumor. Among the welcome negative results were the absence of any indication of cancer or granulomas in my lung tissue.
Once the fever had been handled, a number of the worrisome indicators from my blood tests began to return to more normal levels, and I began to feel more like myself. The hospital’s physical therapy team led me on walks around the hospital floor. Then my wife would take me – on her daily visits from Bloomington bearing food to replace the terrible hospital “room service” – down in a wheelchair once a day to the ground floor to take small walks outside in the fresh air. But several liver enzyme levels in my blood work began to rise rapidly. The ultrasound scan showed no anomalies in my abdominal area, and the gastro-intestinal team doctors seemed reasonably confident that those increases were a side-effect of the antibiotics I’d been on. The liver levels did begin to return to normal levels, but only after three days, which delayed my neurosurgery even longer.
Meanwhile, the first and only positive lab result came back from culture growths on the fluid that had been removed from my lung during the bronchoscopy. That culture had revealed one colony of Streptococcus mitis, a bacterium that normally lives within human mouth, throat and gastro-intestinal regions and is generally considered not very harmful. These bacteria may get transferred to the lungs during episodes of acid reflux, choking or regurgitation, and that would explain why they seemed confined to the upper lung region in my case. But it was not very satisfying to think that not very virulent bacteria from my own gut might have been the root cause of my diverse symptoms. Thus, on May 21, we finally moved ahead to my neurosurgery without a clear explanation of how all my symptoms might have been interrelated.
IV. the surgery
“If you have to have a brain tumor, yours is the one to have.” That’s what Dr. Jesse Savage told me shortly before he performed my neurosurgery. He showed me one of the MRI images of my tumor (see Fig. 8) and explained that it was exerting significant pressure on both the optic nerves and the pituitary gland. Much later, weeks after the surgery, I asked him what the normal diameter of the Sella is, and he told me it is “dime-sized.” My tumor was considerably larger than this and could fit in as it grew by not only squashing the pituitary, but also pushing out the walls of the Sella cavity.
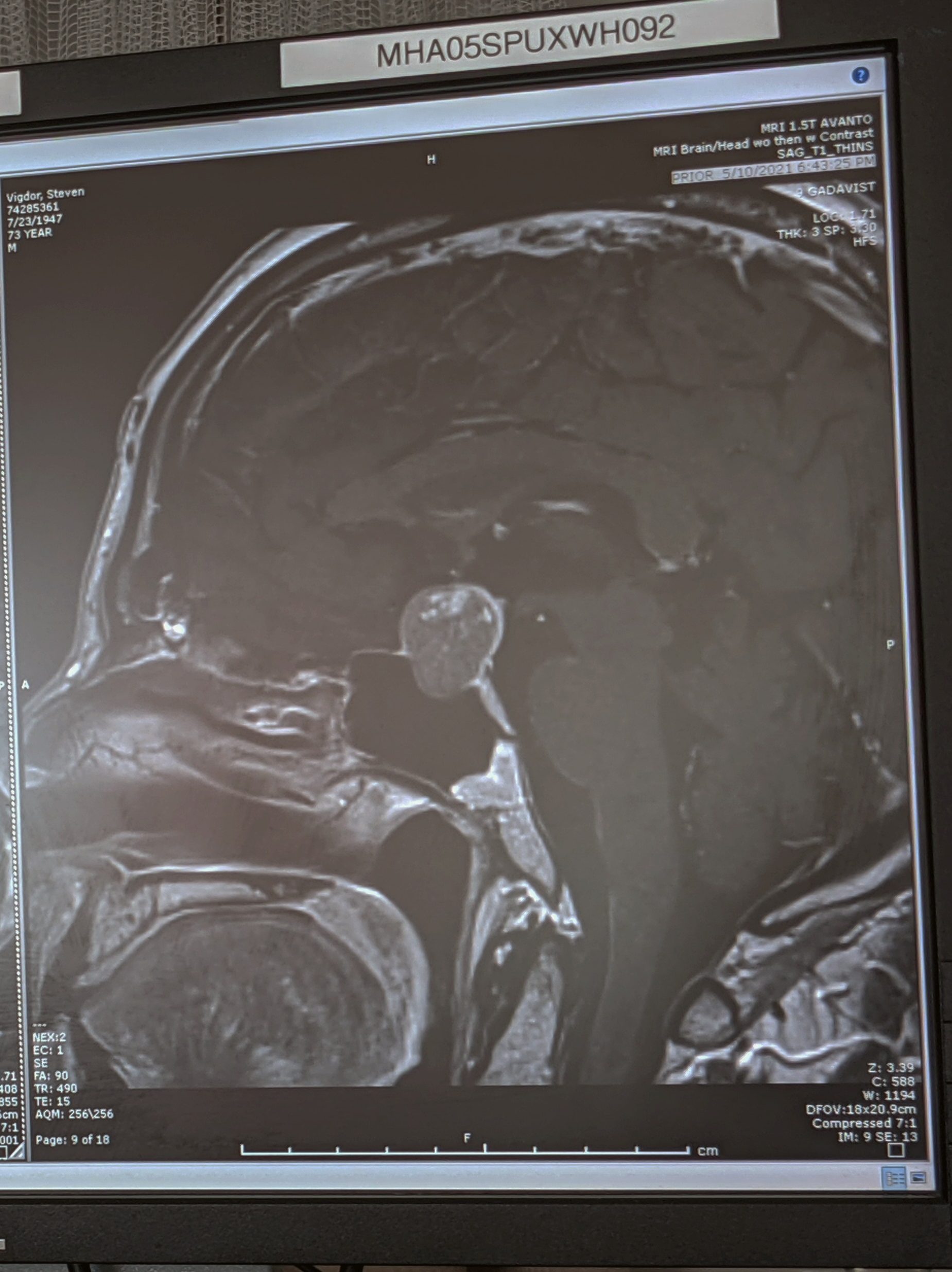
Dr. Savage speculated that the lighter dots near the top of the tumor in Fig. 8 might indicate that the tumor itself had begun internal hemorrhaging. If so, that would make the extraction easier because the tumor matter would be squishy. It might also explain the sudden onset of my symptoms, because hemorrhaging tumors enlarge rapidly, leading to a condition called pituitary apoplexy.
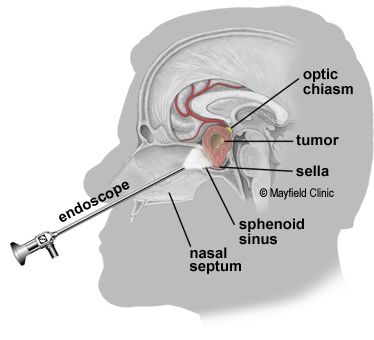
Dr. Savage explained the procedure he was about to perform in more detail than it had been explained to me previously. The procedure was an endoscopic transsphenoidal removal of the tumor through my sinus passages and nose. He assured me that my tumor was intermediate in size compared to the array of tumors he had personally removed surgically via this procedure during his career to date. The procedure is illustrated schematically in Fig. 9. An endoscope with a tiny camera at its end is inserted through one nostril and the nasal and sinus passages to illuminate the surgery to be performed. Through the other nostril the surgeon can insert tools to make small holes in the nasal septum, the sphenoid sinus, and the Sella turcica wall (see Fig. 7) to gain access to and extract the tumor and, if necessary, to repair the holes. The patient remains under general anaesthesia during the procedure, which normally takes 2-3 hours to perform. This may all seem invasive, but it’s much less so than cranial surgery, which would be extremely complicated to address a tumor near the brain stem.
Dr. Savage also forewarned me about the most common collateral problem that arises in this type of surgery. That is damage to the delicate arachnoid membrane that surrounds the brain, leading to leakage of cerebrospinal fluid (CSF). If that occurred, it would require patching the hole at the back of the sphenoid sinus with a graft of fat tissue taken from my belly and some special glue. If a leak occurred, they would also have to insert a needle through my lumbar to allow CSF to drain and relieve pressure that might otherwise force the fluid through my nose.
He also told me what to expect post-surgery. I would awaken with both nostrils plugged with bandages to prevent excessive blood and scar tissue leakage through my nose, and thus have to breathe through my mouth for a day or two. I would spend at least one night in the Intensive Care Unit as they monitored particularly my thirst level, urine output and sodium levels as indicators of another possible collateral effect known as diabetes insipidus. That condition could arise if the posterior lobe of my pituitary gland or my hypothalamus were damaged, as they control the level of the anti-diuretic hormone ADH that regulates thirst and urination. They would want a second MRI scan of my brain and my Sella within three days of the surgery, in order to verify how successful the tumor removal had been. I would experience sinus headaches that might be severe at first and would gradually lessen over 4-6 weeks, as the inflammation caused by the surgery decreased. My peripheral vision and my pituitary hormone levels might return to normal, but also might recover only partially.
Dr. Savage’s clear explanations were very valuable because I was, of course, completely out during the surgery. The first thing I remember after the surgery was being wheeled on a bed to the ICU, with both nostrils plugged as promised. The ICU doctor and nurses said they wanted to schedule an MRI for me that night, but my wife complained bitterly that I was not yet even fully conscious, and that Dr. Savage had requested the MRI only within the ensuing three days. I complained that the hospital air was so dry that my mouth breathing passages were extremely dried out and I didn’t think I could make it through a 40-minute MRI session without needing multiple drinks of water. So the MRI was postponed.
In the aftermath of the anaesthesia I had acid reflux and managed to regurgitate some of what I had eaten earlier in the day. I spent a miserable, largely sleepless, first night in the ICU, with a severe headache – a night made worse by a night nurse who was convinced that the proper monitoring of my urine output required her to not allow me to drink anything. By the next morning Dr. Savage had corrected her misinterpretation, and the ICU nurses were offering me multiple drinks.
Dr. Savage made an appearance on that first morning in the ICU to let me know several things. First was that he thought he had succeeded in removing the tumor in its entirety. It seemed quite firm, so his speculation about an internal hemorrhage within the tumor was incorrect. There had, in fact, been a small breach of the arachnoid, and consequently they did extract belly fat to patch the bony holes and they did have me on a lumbar CSF drain. My urine output, measured via catheter, did not seem particularly elevated, so it was unlikely that I had developed diabetes insipidus. And to my great relief, he removed the bandages blocking my nostrils.
Then, in a ritual to be repeated each following morning in the hospital, he had me sit up and bend my head forward to see whether there was any sign of CSF leakage through my nose. There was not. The second part of the morning ritual involved a neurosurgery team member wiggling fingers far off in the periphery while I covered one eye at a time and stared at his central hand. The qualitative results of that exercise seemed to promise some considerable improvement from pre-surgery in my peripheral vision. Once I was able to breathe through my nose again, I agreed with Dr. Savage that I could have the MRI scan on that day.
At that point, the major after-effects of the surgery were the continuing severe headache (exacerbated by a stiff neck from sleeping with headrest tilted upward on the rather uncomfortable ICU bed) and a loss of appetite. The ICU doctor came in to chat and then declared me alert and awake. I assured her that “awake” was an exaggeration. She insisted that it was important to address the headache pain with medications, but the Tylenol they tried first had no effect. Later that day they administered a dose of fentanyl intravenously, but this too had no discernible effect on the level of headache pain. When the nurses, during my second night in the ICU, offered to try more fentanyl, I refused: “Why would you give me more opiate, when it seems to do nothing to alleviate my pain? The only good news is that I’m unlikely to get addicted to it because there’s probably no dopamine rush if there’s no pain reduction.”
At my wife’s urging I tried to get a little food down during that day in the ICU, but then I regurgitated the acidic parts (orange juice, strawberries) that evening. My wife also brought from home a small, portable humidifier that helped a lot to alleviate my thirst from the extremely dry hospital air, until it was broken by a nurse a couple of nights later. The evening nurse notified me that I might get transported for an MRI scan and/or to a new room in the Post-Care Unit (PCU) later on in the evening. The new room did not become available. But, in keeping with what seemed hospital protocol to interrupt sleep as much as possible for blood draws and medications, they did awaken me at 1:30 am to get my MRI scan. Another 40 minutes of head stillness in a narrow tube with an even louder MRI apparatus than I’d experienced in Bloomington. When the scan was completed, the MRI technician said he’d gotten great pictures and asked how it went for me. I replied “It’s a form of torture, you know.”
After my second ICU night, the ICU doctor returned to try some different approaches to alleviating the headache pain. Cold compresses helped a little, as did lying flat rather than with my head elevated. But the winner was a dose of fioricet, a mixture of acetaminophen, caffeine and butalbital that is particularly effective on tension headaches. My daughter, who had just flown in from Seattle to help my wife handle my recovery, had come to the hospital with food, a neck pillow and other goodies. Shortly after taking my first dose of fioricet, I had asked the day nurse to help me get out of bed and sit in a chair to eat and chat with my daughter. At first, the headache was still severe, but about a half-hour into that session it was like a veil had lifted. My daughter could see the change in facial expressions and said “Well, that seemed to work.” I was now also able to eat and keep down substantially more than I’d managed the previous day.
Since my urine output was still judged within a normal range, the nurse also removed the catheter that day. With the catheter removed and the fioricet making it easier to manage the headache pain, the main issue standing between ICU and my release from the hospital was the lumbar drain and continued evidence that the sphenoidal patch was holding to stop CSF leakage through my nasal passages. My daughter had noticed some leakage around the top of the needle inserted through my lumbar, so a team was sent from the neurosurgery group to add a suture there. They administered fentanyl intravenously to help alleviate the pain of putting stitches in, but they waited only a minute before proceeding, so the sewing was certainly uncomfortable. Furthermore, in a sign of what was to come, my nose started bleeding when I lay on my side during the suture application.
My third overnight stay in the ICU was considerably improved: medical interruptions were limited, the neck pillow, humidifier and fioricet doses every 6 hours kept me more comfortable, and I was finally able to get a semi-decent night’s sleep. My lunch with my daughter the following afternoon was interrupted by a nurse informing me that a room in the PCU was finally available, and I would be transported there shortly. I asked first to try the commode they had provided for me, since I felt my medication-induced constipation lifting. By the time I was done, I was told that in the ruthless competition for scarce available beds, someone else had claimed the available PCU room.
That afternoon I was informed that all signs were positive and the lumbar drain would probably be removed the following morning, allowing my discharge from the hospital that day, May 25. But on the evening of May 24 I began to experience significant sinus drainage of a mixture of phlegm and blood. I was told this was normal and not to be concerned unless there were evidence of CSF leakage in what I was spitting up. So I tried to sleep, but was then awakened at midnight to transport me to a PCU room that had just become available. Communication between the ICU and PCU nurses was apparently imperfect, because when I requested a vessel for sinus drainage in the PCU, the nurse said she had heard nothing about that. She did finally, after some discussion, provide a rather large, unwieldy cup, which I managed to inadvertently knock over in the middle of the night. It took 15 minutes before anyone responded to my use of the call button to request someone to clean up the significant spilled blood.
By morning I developed a nosebleed that would not seem to stop. The PCU day nurse asked whether anyone from the neurosurgery team had told me this was normal. I said yes, but I hadn’t been expecting it to be so unstoppable. She replied “Well, that’s frustrating,” and turned to leave. Having expected a reply more along the lines of “Let’s see what we can do to help,” I answered “Thanks,” in what must have come across as a somewhat sarcastic remark.
The doctor who came to remove the lumbar drain hesitated when she saw the ongoing nosebleed and said she would have to consult first with Dr. Savage. A neurosurgery intern, and then Dr. Savage, came to my room to inspect. By that time, I had managed to slow the nosebleed. Each of them explained that it was difficult to stop the blood flow because of the blood thinners that I’d been given every day while in the hospital, to prevent deep vein thrombosis and a possible pulmonary embolism while I was confined to bed. Each of them had me lean my head downward and confirmed that there was still no sign of CSF leakage. Therefore, Dr. Savage authorized the removal of the lumbar drain.
While he was there, Dr. Savage showed me the post-surgery MRI, which indeed showed no sign of any tumor remnants. He indicated he would probably request a follow-up MRI for me in 6 months, noting that I had made clear how much I disliked the lengthy and overloud MRI scans. He asked whether I was ready to be discharged or preferred to spend another night in the hospital. I replied, “Look, the hospital is the right place to be for surgery, but it’s no place to get well. I’m more than ready to leave.” He concurred with my assessment. So, the lumbar drain stitches were removed along with the drain, and I was authorized for discharge, pending concurrence from the physical therapy team. I had walked around the ICU easily with a member of the physical therapy team on each of the previous two days, and did again around the PCU on the afternoon of the 25th, also climbing up and down a few stairs several times, and they readily agreed that a discharge was in order.
I got a small hint that the PCU nurse was as eager to see me go as I was to leave the hospital. She took me downstairs in a wheelchair while my wife drove up to the circular entrance to the hospital. Before my wife arrived, the nurse’s cell phone rang. She explained to the caller: “I’m downstairs getting ri…uh, discharging a patient.”
V. Recovery and assessment of what had caused my symptoms
It was very good on multiple levels to return home after a 15-day unanticipated hospital stay. My daughter was still in town, on her next-to-last day, and my elder son arrived, also from Seattle, on the evening of my discharge. The love they and my wife showed me was warming, and so was the opportunity to interact with my family in a home setting. That interaction gave me confidence that I would return to my old, punning self, with the same selective memory of two or three lyrics from almost every tune written before 1970. As I texted my sister: “The good news is that the surgery was successful. The bad news is that there will be no personality change.”
There is no universal agreement in the medical community about the optimal post-surgery care following removal of a pituitary adenoma. But I left the hospital with a number of restrictions on what I could do as well as prescriptions for several medications I would need during the 4-6 weeks of recovery following surgery. Among the restrictions: don’t bend so that your head is below your heart; don’t blow your nose; don’t drink from straws; don’t lift anything weighing more than ten pounds; don’t load or unload the dishwasher if it requires bending.
I also couldn’t drive yet, although I’ve been authorized to do so by this writing. So, on my third day at home, my wife drove me and my son to the barriers I’d told her I drove through before parking my car on May 10. She wanted to prove to me that I must have misremembered my path, but my son got out of the car and confirmed that it was just possible to squeeze my car through if it was perfectly aligned. As I had told them, it was an irrational decision, but precisely executed. Meanwhile, my younger son remained at his home in Seattle, but engaged me in testing new software he is developing. That at least made me feel a bit useful under the restriction regime.
Most prominent among the prescriptions was hydrocortisone, which had been administered at first intravenously in the ICU, and then reduced to pills by the time of my discharge. This prescription was intended to boost my body’s production of the stress hormone cortisol, as my pituitary gland hopefully recovered from its tumor-weakened state. A Google search indicated the central role cortisol plays in governing the body’s responses to physical or mental stress. Its enhanced production during stressful episodes affects multiple aspects of metabolism and immune system function, for example, to allow the body to fight off infections or inflammation, and to increase glucose production and energy to fuel “fight-or-flight” responses to threatening stimuli.
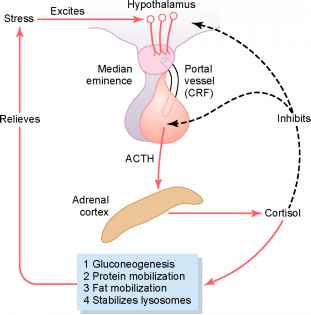
Cortisol is released directly by the adrenal glands just above the kidneys, but the pituitary gland plays a central role in stimulating and regulating cortisol production. As indicated in Fig. 10, a stressful stimulus excites the hypothalamus to secrete a peptide called corticotropin-releasing factor (CRF) into the anterior pituitary gland, which then, in turn, sends a signal to the adrenal glands via release of adrenocorticotropic hormone (ACTH). Upon receipt of the ACTH, the adrenal gland responds by increasing cortisol production to manage and hopefully relieve the stress. But the enhanced cortisol levels in the blood are sensed to provide negative feedback signals to the hypothalamus and the pituitary gland, to inhibit further ACTH and cortisol production once the stressful stimulus is successfully managed. This self-regulation is important to prevent the harmful effects of prolonged excess cortisol levels, which can include weight gain, high blood pressure, muscle weakness, and diabetes.
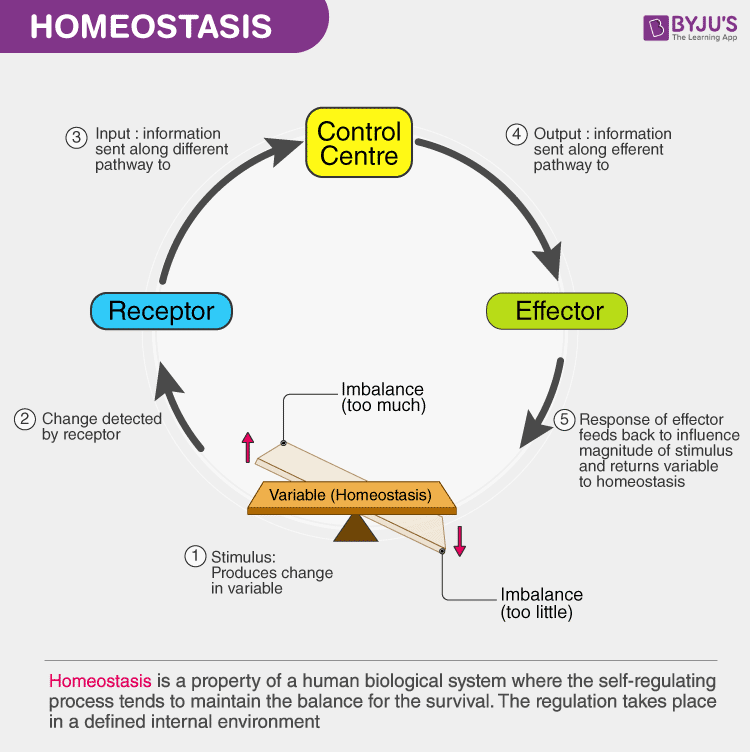
The self-regulation of cortisol production is just one example of the role the hypothalamus plays more generally in maintaining the metabolic balance, or homeostasis, the body needs for long-term survival. It provides the brain’s control center in the generic feedback loop illustrated in Fig. 11, sending chemical signals to return the body’s levels to equilibrium after that balance is upset by an external stimulus. When homeostasis relies on hormonal balance, the pituitary is the intermediary for receipt and transmission of those signals.
The anterior lobe of the pituitary gland governs the secretion of cortisol, reproductive hormones such as testosterone and estrogen, thyroid hormones, growth hormone, follicle-stimulating hormone, and prolactin, which stimulates production of breast milk in women. The posterior lobe secretes the anti-diuretic hormone (ADH) that controls water retention by the kidneys and oxytocin, which affects uterine contractions during pregnancy. When I entered the hospital, my levels of cortisol and testosterone were both quite low, indicating that the anterior pituitary was adversely affected by the tumor. The absence of diabetes insipidus after my surgery suggested that the posterior lobe, if it had been affected, had returned to something close to normal ADH production.
The hypothalamus is also central in maintaining the body’s circadian rhythm. In the absence of stressful external stimuli, the healthy body adjusts cortisol production throughout the day, keeping the level low during the night to facilitate restful sleep, and raising it rapidly in the morning to increase wakeful alertness. Nighttime sleep is also facilitated by darkness-induced melatonin secretion from the pineal gland located within a groove where the two halves of the thalamus join.
Under-production of cortisol can lead to a variety of symptoms, prominently including fatigue, weakness and low blood pressure. When the anterior pituitary lobe is damaged and leads to ACTH levels as low as mine were upon entry into the hospital, the body can experience an Addisonian crisis when subjected to stress. Among the symptoms of such an episode are dizziness, mental confusion, fever, chills, and a reduced resistance to infection. Check, check, check, check and check: these describe my state at the time of the fall that triggered my initial entry into the Emergency Room.
Once I was home, my brain put me through a series of anxiety dreams that seemed designed to drive home the buildup of stress that could be caused by failure to perform even simple tasks under time pressure, in the absence of sufficient cortisol. After a first night featuring quite vivid, but enjoyable, dreams, the anxiety dreams began on the second night. I awoke quickly from the first such dream, which featured an exam with incomprehensible questions, reminding myself that I did not have to take any more exams in my life.
So, my brain substituted taking over chairmanship of a Physics Department, as I had done twenty years earlier at Indiana University, but now in an emergency situation, and despite my protestations that recent brain surgery meant I could not make such a commitment. I had to begin the tasks of chairmanship immediately, but could do so only after I completed seemingly trivial tasks: in one dream, dressing up for dinner with faculty, but using only ill-fitting and mismatched clothes left in my office; in another dream, filing travel expenses for which I had no records and couldn’t even locate printer paper to output a spreadsheet. Both times I began to panic and failed to complete the simple tasks, much as I had failed on May 10 to locate a COVID testing site I was told I couldn’t miss. I awoke from those dreams convinced that my serious ACTH and cortisol shortfall, caused by the pituitary adenoma, had been the root cause of most of my diverse symptoms.
It still remains unclear why my symptoms seemed to begin suddenly toward the end of our Arizona vacation. Had the tumor simply grown gradually to the point where it exerted sufficient pressure on the optic nerves and the pituitary to attract my attention? Was its growth rate rather enhanced by the onset of hemorrhaging within the tumor, or alternatively by the tumor outgrowing its blood supply? Might its growth rate have been affected by either the altitude or the intense heat we experienced in Arizona?
The ophthalmologist who oversaw my follow-up eye exam post-surgery told me “You’ll probably never find out the reason for the sudden onset of symptoms.” The field-of-vision tests in that follow-up exam revealed that with the tumor removed my peripheral vision had partially recovered, with remaining blind spots in the near periphery on opposite sides in my two eyes. There may be some continuing recovery, but the remaining vision issues are unlikely to cause noticeable problems, as my brain adapts to the new situation and I learn to move my head and eyes to assess potential hazards on the ground in front of me.
As I write this post, I am more than halfway through my projected recovery. The sinus headaches are still present, but have steadily decreased in intensity, as promised. In consultation with my endocrinologist, we’ve been reducing the morning and afternoon hydrocortisone dosage in stages to see how my body and my sleep patterns respond. For the moment, I tend to sleep in roughly one- to two-hour segments, after which falling back asleep is easy on some nights, but not on others. A follow-up blood analysis three weeks after the surgery has shown that ACTH levels from my pituitary gland remain quite low. The hydrocortisone can replace the pituitary’s role in cortisol production only partially, because it bypasses the self-regulation feedback loop illustrated in Fig. 10. This means that when the body is stressed physically or mentally, I will have to increase the dosage manually to approximate how a healthy pituitary gland might have responded, and then decrease it again when the stress is relieved. I also remain on a low dosage of thyroid hormone.
I have just had a follow-up visit with my neurosurgeon, Dr. Savage. He assured me that the biopsy report on the tumor tissue removed showed that it was benign, as are the overwhelming majority of pituitary adenomas. While benign, they do often reappear and grow again. So I will have to have follow-up MRI scans periodically over the coming years. Dr. Savage considered my recovery to be going well, and he removed most restrictions on my activities, so that I can resume feeling fully functional. This is good because my wife is tiring of mowing the lawn in my place. On the other hand, Dr. Savage also indicated that full recovery of pituitary function and sinus health can take up to a year. Recovery from brain surgery requires patience.
VI. take-aways
My extended hospital stay and ongoing recovery have triggered or reinforced several general perceptions:
- Every experience one has, whether positive, negative or neutral, presents a learning opportunity. I have enjoyed researching some aspects of brain function as I try to piece together the causes and symptoms of my distress. I am likely to add some future blog posts on other aspects of brain function and manipulation in the current media environment.
- One should not take one’s health or brain function for granted. Be alert to changes that appear serious and get medical assessments promptly. My fall and entry into the Emergency Room, while unfortunate, probably presented the quickest path to a diagnosis of the underlying issues. Pituitary adenomas are not uncommon, but most escape detection until they grow to macro size, because brain scans are not often performed.
- The past 15 months of COVID-19 pandemic have taken a serious toll on the nation’s nursing corps. Departures have led to significant understaffing during my hospital stay. And the nurses who remained, many of them caring and competent, appeared to me to make too many mistakes. The last words a patient wants to hear from a nurse following one among many blood draws are “Oops” (forgot to get all the requested samples) or “Did I just really throw away that blood sample?” Yet I heard both of those. Another blood draw gave flawed results when a nurse tried to use my ever-present blood pressure cuff in place of the usually applied tourniquet. Other nurses simply missed veins on the first one or two tries. Response times to call buttons, sometimes for urgent reasons, often ran to 15 or 20 minutes. Other nurses sometimes delivered such a stream-of-consciousness narrative about their days, their lives and their other patients that it was difficult to discern the reason for their entry into my room.
- The advances in medical technology are impressive. I am still sort of amazed that a one-inch tumor can be removed through one’s nostrils, with precise guidance from a tiny endoscopic camera. The procedure is nothing like the image I had of brain surgery before I entered the hospital. MRI scans represent a critical, high-resolution application of a long-established technique (nuclear magnetic resonance) in basic nuclear physics research. Noiseless MRI imagers are now commercially available, though not used in the hospitals where I spent time. On a more general note, nearly everyone is content to embrace advances in technology, but still many people insist on distrusting the science underlying those advancements, if that science appears to threaten their worldview. That distrust and science denial is, after all, the motivating factor behind this blog site.
- The brush with a serious medical condition led me to contemplate my epitaph during my hospital stay. Since W.C. Fields had already taken “On the whole, I’d rather be in Philadelphia,” I decided to adapt a cheerful comment made about halfway through my hospital stay by a nurse practitioner on her daily rounds, while she was listening through a stethoscope positioned on my abdomen: “Loving husband and father. He had great bowel sounds.” That about sums it up.
references:
K. Sukel, Neuroanatomy: The Basics, https://dana.org/article/neuroanatomy-the-basics/
https://teenbraintalk.wordpress.com/limbic-system/
M.G. Lake, L.S. Krook and S.V. Cruz, Pituitary Adenomas: An Overview, American Family Physician 88, 319 (2013), https://www.aafp.org/afp/2013/0901/p319.html
https://www.yourhormones.info/glands/pituitary-gland/
https://www.pituitary.org.uk/information/hormones/
https://en.wikipedia.org/wiki/Cortisol
https://www.webmd.com/brain/empty-sella-syndrome-facts
Pituitary Tumors, https://www.mayoclinic.org/diseases-conditions/pituitary-tumors/symptoms-causes/syc-20350548
Endoscopic Pituitary Surgery (Transsphenoidal), https://mayfieldclinic.com/pe-endopitsurg.htm
Pituitary Adenomas, http://pituitary.ucla.edu/pituitary-adenomas
A. Prete, S.M. Corsello and R. Salvatori, Current Best Practice in the Management of Patients After Pituitary Surgery, Therapeutic Advances in Endocrinology and Metabolism 8, 33 (2017), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5363454/pdf/10.1177_2042018816687240.pdf
K. Boyd, Visual Field Test, https://www.aao.org/eye-health/tips-prevention/visual-field-testing
https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/bronchoscopy
https://www.mayoclinic.org/diseases-conditions/valley-fever/symptoms-causes/syc-20378761
https://www.mayoclinic.org/granuloma/expert-answers/faq-20057838
S. Sethi, Community-Acquired Pneumonia, https://www.merckmanuals.com/home/lung-and-airway-disorders/pneumonia/community-acquired-pneumonia
Antibiotics and Liver Injury – Be Suspicious!, https://www.medsafe.govt.nz/profs/PUArticles/AntibioticsSept2012.htm
A. Sapkota, Streptococcus Mitis – An Overview, https://microbenotes.com/streptococcus-mitis/
Pituitary Apoplexy, https://medlineplus.gov/ency/article/001167.htm
https://en.wikipedia.org/wiki/Arachnoid_mater
https://en.wikipedia.org/wiki/Cerebrospinal_fluid
Extended CSF Drainage Trial Via Lumbar Drain, https://www.hopkinsmedicine.org/neurology_neurosurgery/centers_clinics/cerebral-fluid/procedures/csf_drainage_trial.html
Diabetes Insipidus, https://www.mayoclinic.org/diseases-conditions/diabetes-insipidus/symptoms-causes/syc-20351269
https://www.healthline.com/health/adh
Fentanyl, https://medlineplus.gov/druginfo/meds/a605043.html
Fioricet, https://www.webmd.com/drugs/2/drug-15869/fioricet-oral/details
Deep Vein Thrombosis (DVT), https://www.mayoclinic.org/diseases-conditions/deep-vein-thrombosis/symptoms-causes/syc-20352557
Hydrocortisone, https://medlineplus.gov/druginfo/meds/a682206.html
Regulation of Cortisol Secretion by Adrenocorticotropic Hormone from the Pituitary Gland, https://www.euroformhealthcare.biz/medical-physiology/regulation-of-cortisol-secretion-by-adrenocorticotropic-hormone-from-the-pituitary-gland.html
High Cortisol Symptoms: What Do They Mean?, https://www.healthline.com/health/high-cortisol-symptoms
https://byjus.com/biology/homeostasis/
https://en.wikipedia.org/wiki/Circadian_rhythm
https://en.wikipedia.org/wiki/Pineal_gland
Addisonian Crisis (Acute Adrenal Crisis), https://www.healthline.com/health/acute-adrenal-crisis
https://en.wikipedia.org/wiki/Nuclear_magnetic_resonance
Michigan Hospital First to Install Noiseless MRI System, Sept. 24, 2013, https://www.itnonline.com/article/michigan-hospital-first-install-noiseless-mri-system
