
05/11/2026
I. INTRODUCTION
On March 31, 2026 the U.S. Supreme Court ruled that a Colorado state ban on conversion therapy for minors raised significant issues vis-à-vis First Amendment free speech rights when it comes to talk therapy. Conversion therapy, in general, comprises a variety of methods used in attempts to change an individual’s sexual orientation, if it involves same-sex attraction and/or behaviors, or gender identity, if it differs from the person’s biological sex as determined by reproductive organs. The approach is sometimes called reparative or reintegrative therapy.
Psychological, psychiatric, and medical studies of individuals who have undergone conversion therapy have found little evidence that sexual orientation actually changes over the long term and that conversion therapy often may induce psychological stress and harm, including suicidal tendencies. For these reasons, Colorado passed a 2019 state law banning licensed professionals from practicing conversion therapy on minors. The Alliance for Therapeutic Choice and Scientific Integrity (ATCSI), a U.S. organization that promotes conversion therapy, publishes The Journal of Human Sexuality primarily to provide countervailing evidence that the therapy succeeds in changing sexual orientation. ATCSI strongly supports the new SCOTUS ruling.
The SCOTUS ruling deals only with talk therapy, as opposed to physical or coercive conversion techniques. It identifies talk therapy as a form of speech and remanded the case back to lower courts to decide whether Colorado had a compelling state interest in denying this form of protected speech.
In this post we will survey the history and character of various conversion therapy approaches, the evidence regarding their efficacy and dangers, the attitudes toward them of professional medical associations and human rights organizations, and the current legal status of conversion therapy in the U.S. and other countries. But we begin by discussing the evolution of scientific thought and the contrast with conservative religious thought about human sexual orientation and gender identity.
Scientific understanding of human sexual orientation and gender identity has evolved considerably over the past half-century, while still remaining incomplete. The American Psychiatric Association first identified homosexuality as a mental illness in 1952 in the first edition of the Diagnostic and Statistical Manual of Mental Illnesses (DSM-I), categorizing it as a “sociopathic personality disturbance.” The categorization remained in DSM-II in 1968, but was then removed from the manual in 1973, after some scientific review and a considerable amount of activism, although “sexual orientation disturbance” remained. It was finally eliminated completely as a mental disorder in DSM-III in 1987 and by the World Health Organization in 1990.
Gender identity disorder was formally included in DSM-IV in 1994 (replacing transsexualism in DSM-III), but softened to gender dysphoria in DSM-5 (2013) to shift the focus from unconventional identity to the distress experienced by many affected individuals. The American Psychological Association now distinguishes between conversion therapy addressing sexual orientation (Sexual Orientation Change Efforts, or SOCE) vs. gender identity (Gender Identity Change Efforts, or GICE). Most professional organizations argue against the use of the term “conversion therapy” because they now believe that there is no medical or psychological disorder being treated and that the efforts have not shown any indication of being therapeutic. While we accept that judgment, we will continue in this post to use the conversion therapy term because in popular understanding it is used as an umbrella term encompassing an array of techniques that have been applied in attempts to alter sexual orientation and gender identity.
We will discuss briefly below what is currently known about the biological underpinning of these conditions. But first we note that for many religious institutions the situation is clear-cut: same-sex orientation and gender dysphoria are seen as sinful because they deviate from the focus on male-female procreation, among both humans and animals, in scripture. Same-sex genital arousal and even, rarely, long-term mating has been observed in the wild among numerous animal species, including several primate species. Conservative theology assigns humans free will to choose or reject sinful behavior. Therefore, conservative religious institutions see same-sex attraction among humans as a particularly sinful choice, rather than a biologically determined and immutable human characteristic. Certain passages in the Judaeo-Christian Bible explicitly identify same-sex attraction as an “abomination” or “contrary to nature.” Some conservative religious organizations attribute homosexuality to environmental influences, trauma, or rebellion, but not to immutable biology. If it is an exercise of free will, then these organizations argue that it should be subject to change with suitable supervision. This belief has largely motivated the history of conversion efforts that we will survey in Section II.
Evolution would seem to require the same focus on male-female sexual reproduction. Successful and fecund reproduction – i.e., propagation of the species — is, of course, the metric by which successful biological evolution is judged. It is thus non-intuitive that evolution might have yielded some sexual behavior that cannot result in reproduction. But the way biology incentivizes the evolutionary pressure toward reproduction is by inducing sexual attraction and arousal and rewarding sexual release by dopamine secretion in the brain’s reward pathway. And the allure of sex – the sense of well-being triggered in the brain’s reward system — leads to a great deal of human (and animal) sexual interactions that are not aimed at reproduction.
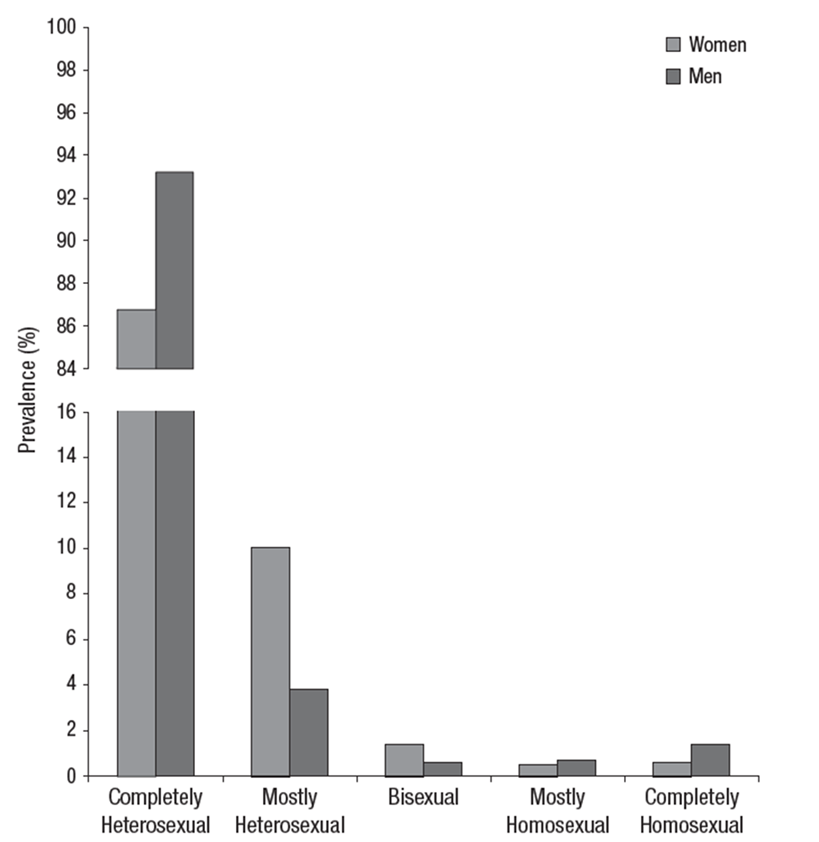
A species in which exclusive same-sex attraction or gender identity deviating from reproductive-organ sex becomes dominant would be evolutionarily doomed. But when these behaviors represent minority divergences along a spectrum of sexual and gender orientation – surveys in Western countries have generally shown fewer than 5% of respondents with predominantly same-sex attractions (see, for example, Fig. I.1) – they may just represent the price a species pays for evolution driven by imprecise genomics or subject to poorly controlled environmental (epigenetic) effects on gene expression.
For example, Jenny Graves speculates that there are alleles on chromosomes shared between men and women that enhance either “male-loving” or “female-loving.” When a male-loving allele occurs in men it favors homosexuality to some degree, but the same allele in women may predispose the affected individuals to mate earlier and have more children, thus offering an evolutionary advantage. A similar evolutionary advantage may occur in men who have the female-loving allele, while in women that allele favors lesbianism. Indeed, an Italian study found that maternally inherited (thus, likely X-chromosome) alleles enhanced both female fecundity and male homosexuality. They found that in their sample female relatives of gay men have 1.3 times as many children as the female relatives of straight men.
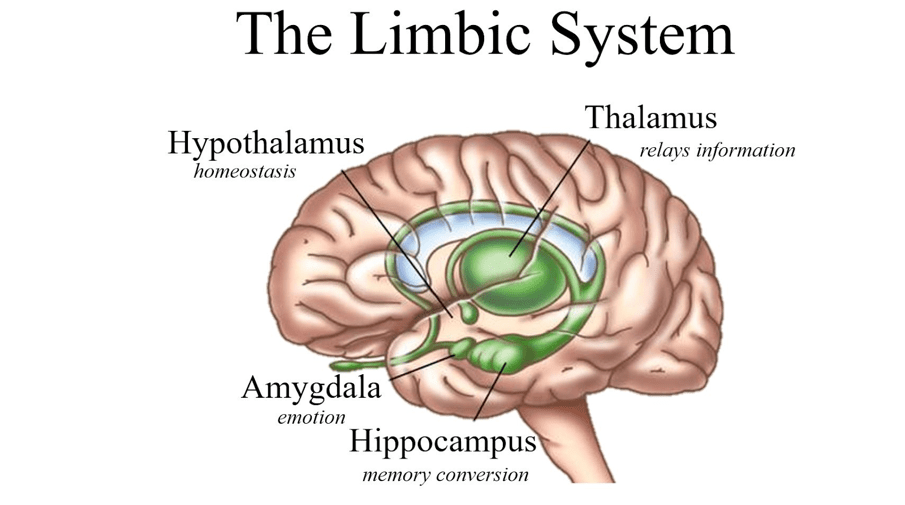
Scientific study of the biological origins of sexual preferences and gender identity is far from complete. But results to date indicate the involvement of specific brain regions, neural pathways, neurotransmitters, and hormones. There is evidence that human sexual preferences are influenced most strongly deep inside the brain in the limbic system (see Fig. I.2) that lies beneath the temporal lobe of the cerebral cortex. Primary evidence is derived from a meta-analysis of neuroimaging data obtained via functional MRI and PET techniques from a combined sample of 364 human subjects – including both males and females, encompassing “healthy hetero- and homosexual individuals as well as individuals with gender identity and sexual preference disorders (i.e., transsexualism and pedophilia).” The imaging reveals brain regions activated when subjects were exposed to visual and/or olfactory stimuli representative of the subject’s preferred or non-preferred sexual partners.
The brain regions that show up most systematically in these imaging studies are the following:
- The hypothalamus, in particular, the anterior and preoptic sections. The hypothalamus regulates much of the hormone secretion within the human body and thereby controls body temperature, hunger, thirst, fatigue, sleep, circadian rhythms, and attachment behaviors. A tiny part of the hypothalamus called the third interstitial nucleus of the anterior hypothalamus, abbreviated as INAH-3, appears to be particularly implicated in controlling sexual attraction in humans. In the 1990s the British-American neuroscientist Simon LeVay examined the brains of recently deceased heterosexual and homosexual men, as well as several heterosexual women. LeVay found “that the INAH3 in the brains of heterosexual men were more than twice as large as that found in the homosexuals. In fact, the INAH3 size of the homosexual group was the same size as the women.”
- The anterior and mediodorsal nuclei of the thalamus, which helps to integrate sensory, emotional, and motivational signals within the brain. Structural MRI imaging reveals gray matter volume differences in the thalamus between the brains of heterosexual and homosexual individuals.
- The septal region of the limbic system, which is involved in reward, bonding, and pleasure recognition within the brain.
- The amygdala, which determines the emotional salience of stimuli, including sexual cues. Amygdala connectivity patterns in homosexual individuals are atypical for the individual’s sex.
- Regions of the hippocampus show up clearly when subjects with pedophilic preferences are included in the human sample but are not present at a statistically significant level otherwise.
Poeppl, et al.,speculate that “The lack in involvement of cognitive cortical regions may in addition account for the immutability of sexual preferences…[and]… supports the view of an in utero determination of sexual preference during early fetal development… Neural networks underlying psychosexual arousal however involve also the lateral prefrontal cortex and superior parietal lobules, which have been implicated in top-down control in this context. This neural specificity of the sexual preference network within the psychosexual arousal network could furthermore explain why sexual arousal can be contained, while sexual preference per se is not subject to deliberate control.”
Fetal brain development also appears to be critical in the formation of an individual’s gender identity. The sexual differentiation of male from female brains begins during a testosterone surge during the second trimester of pregnancy. Differences show up in both grey matter, where the brain’s processing is done, and white matter, which provides the communications between different parts of the brain and between the brain and the body. The white matter is so-called because it contains many nerve fibers or neurons that are sheathed in the white fatty insulating protein called myelin. The prenatal testosterone surge appears to be responsible for the systematic male-female differences in the size of the INAH-3 section of the hypothalamus. In addition, neuroimaging studies on many men and women have revealed the typical differences in white matter connections illustrated in Fig. I.3.
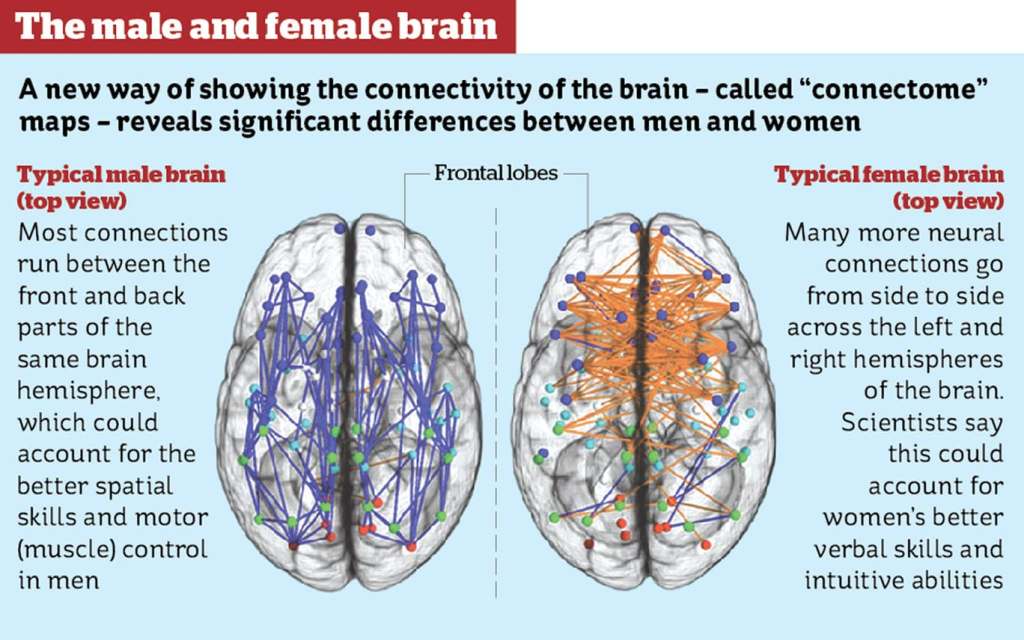
Gender dysphoria arises when an individual’s sense of gender, determined in the brain, is not well aligned with the sex organs formed during the first trimester of pregnancy. According to Debra Soh, brain imaging on adult transgender men and transgender women who were not currently taking hormone supplements (which might, in principle, have affected results) reveal that the transgender adults, in comparison with non-transgender control participants, “have typical [for their birth sex] gray matter volumes (or cell bodies), but differences in white matter (connective tissue)…Transgender women demonstrated a white matter trend in between women and men… suggesting that their white matter tracts were only partially masculinized during development. A similar trend was seen in transgender men [showing] a brain connectivity pattern closer to people who shared their gender identity (that is, men) than those who shared their birth sex (that is, women).”
Such sex-atypical white matter connectivity patterns may also play a role in the formation of non-heterosexual orientation. A number of studies have shown that childhood gender nonconformity – behaving like the other sex, well before the recognition of sexual attraction or the onset of sexual activity – is strongly correlated with adult same-sex attractions. This view also receives some support from animal studies on mice, rats, and ferrets, in which testosterone has been either deprived of males or significantly increased for females at early stages of development. These changes led to adult sexual behavior that is more typical of the opposite sex.
There is, then, a fundamental difference in the views of homosexuality and gender identity issues between conservative religious institutions and neuroscience. The former view these conditions as matters of sinful choice subject to social influences while the latter view them as immutable characteristics determined largely during fetal brain development. While neither view is yet definitively proven or refuted by existing studies, the majority of evidence strongly supports the biological origin.
In this post we will review the history (Section II) and efficacy and dangers (Section III) of various types of conversion therapy. But we note that the combination of the relevant neuroscience research and indications of psychological damage induced by at least some forms of conversion therapy have led to statements condemning conversion therapy issued by many professional medical, psychiatric, and human rights organizations. We will review some of these in Section IV. Furthermore, bans on the performance of conversion therapy, at least on minors, have been enacted in numerous countries, states, and cities. We will review the legal status of such bans and court challenges to the bans in Section V.
II. A BRIEF HISTORY OF CONVERSION THERAPY
The idea of ‘conversion therapy,’ or “attempting to change an individual’s sexual orientation, romantic orientation, gender identify or gender expression to align with heterosexual and cisgender norms,” began with the growth of psychoanalytic theory. Before that time, homosexuality was considered a criminal offense, as it still is today in some African countries. In that case, homosexuals could be jailed; or in other circumstances, male homosexuals might be castrated. Modern efforts to “convert” gays from homosexual to heterosexual began with the advent of psychoanalysis in the late 19th century.
In this Section, we will briefly review “explanations” for the origin of homosexuality that arose from psychoanalytic theory. Since psychoanalysts claimed that they understood the origin of homosexuality, this led directly to claims that they could “cure” homosexuality by addressing the trauma they believed was responsible for this “condition.” At this point in time, homosexuality was considered aberrant by society. Many religious groups considered it a sin. They attempted to deal with it by urging gays to confess their sins and vow to repent. Since psychologists claimed to understand the origin of homosexual behavior, various forms of treatment were employed to achieve a “conversion” to a “normal” sexual state. Finally, since homosexual acts were illegal in the U.S. at this time, some homosexuals were imprisoned. We will also discuss the situation in the United Kingdom, where people convicted of “gross indecency” were offered the choice of prison or to undergo what was called “chemical castration.” The two most famous Britons convicted of “gross indecency” were Oscar Wilde in 1895 and Alan Turing in 1952. Wilde was sentenced to two years’ hard labor, while Turing accepted chemical castration as an alternative to prison.
How conversion therapy began and expanded:
Psychoanalysts considered homosexuality to arise from abnormal conditions in early childhood, although different analysts ascribed different “causes” of gay behavior. This led to claims that psychoanalysts could, through the application of the appropriate interventions, “cure” people of homosexuality and change their behavior to that of a “normal” heterosexual. In addition to undergoing psychoanalysis, many gays were either persuaded or coerced into undergoing different interventions. As we will show, a number of these methods were brutal and caused great physical harm. But psychological analysis also produced lasting harm to homosexuals. It is for this reason that virtually every medical association has today expressed strong opposition to conversion therapy efforts. In Section IV we will review statements from several professional organizations that firmly oppose the use of conversion therapy on minors.
Various Conversion Therapy Methods:
Over the years, a number of different methods have been used in order to “convert” homosexuals to a heterosexual state. With the growth of psychoanalytic theory, homosexuality was considered by many to be a psychological reaction, in many cases to be a result of bad parenting. Contemporary research indicates that homosexuality is generally the result of atypical architecture of the brain such that the individual is attracted primarily to people of the same sex. In that case, psychological “explanations” of homosexual behavior are seen to be simplistic hypotheses claiming that this condition arises from abnormal experiences in early childhood development. In Section III of this post we will review research on the efficacy and dangers of conversion therapy to show that such techniques are almost never “successful,” and that they often produce lasting trauma and harm to individuals subjected to these techniques.
Sigmund Freud:
As the father of psychoanalysis, Sigmund Freud (shown in Fig. II.1) had what we would consider today a rather rational and tolerant view of homosexuality. In his opinion, homosexuality was neither an illness nor a neurotic condition. From his experience with patients, Freud believed that most gay people who consulted him wanted to be heterosexual in order to avoid the disapproval of their families and society; Freud believed that this was a superficial motive for change.
In 1935, Freud was contacted by a mother who wanted her son to be treated. Freud wrote to her: “I gather from your letter that your son is a homosexual. … it is nothing to be ashamed of, no vice, no degradation; it cannot be classified as an illness; we consider it to be a variation of the sexual function, produced by a certain arrest of sexual development. … By asking me if I can help [your son], you mean, I suppose, if I can abolish homosexuality and make normal heterosexuality take its place. The answer is, in a general way we cannot promise to achieve it. In a certain number of cases we succeed in developing the blighted germs of heterosexual tendencies, which are present in every homosexual; in the majority of cases it is no more possible. It is a question of the quality and the age of the individual. The result of treatment cannot be predicted.”
Freud’s contention that homosexuality was neither an illness nor a neurosis was not shared with many psychoanalysts of the time. They proposed and carried out a number of different interventions. In this, psychologists were aided by the medical profession; until 1973, when the DSM was updated to eliminate the statement that homosexuality was a personality disorder, many doctors and researchers used extreme methods in an attempt to “get the gay out.” We will list some of them below.
Psychoanalysis of Gays: Many analysts subjected their patients to sessions of analysis designed to eliminate homosexual desire and behavior. For example, some analysts held that homosexuality resulted from unsuccessful passage through the “oral and anal” stages of development. Analyst Melanie Klein wrote a book in 1932 claiming that a gay man could be converted to a heterosexual by reversing paranoia that developed as an infant. And Freud’s daughter Anna Freud asserted that homosexuals suffered from repressed fears of castration, which could be “cured” by a course of analysis. Other analysts claimed that hypnosis could effect a cure. In the 1950s, Edmund Bergler insisted that the cause of homosexuality was due to a dominant mother combined with an absent father. This, he said, led to the development of repressed masochism. Bergler claimed 90% success rate treating gays who wanted to change and who received the right therapeutic approach (i.e., his). However, we now know that Bergler’s methods were unprofessional: he bullied his patients mercilessly, called them liars and told them they were worthless. Bergler engaged in a long-running feud with Alfred Kinsey. Because Kinsey, the leading researcher on sexual behavior, claimed that homosexuality was relatively normal and not pathological, Bergler asserted that Kinsey was making it difficult or impossible for Bergler to “cure” gays.
Castration: The use of castration as either a “cure” or a punishment for homosexuality goes back several centuries. But in the early 20th century physiologist Eugen Steinach theorized that testosterone determined one’s sexuality. His solution for the issue of male homosexuality was to castrate the individuals and then transplant “normal” testicles, justified by the assertion that the presence of “normal” testosterone would result in a cure for homosexuality. However, at that time the immune system would reject transplanted testicles. So this process was eventually abandoned, as it was not only ineffective but often extremely harmful to the individual. While contemporary neuroscience research suggests that prenatal testosterone levels may indeed play a role in determining sexual attraction, it is the effect of testosterone on fetal brain development, not on testes.
A technique employed in the UK in the 1950s and 1960s was to offer a choice to homosexual men who were convicted of “gross indecency,” or same-sex sexual acts. They could either go to prison, or they could undergo “chemical castration;” this generally involved taking drugs like stilboestrol. Stilboestrol is a hormone that was once given to women suffering difficulties during pregnancy or following a miscarriage. It is no longer in use as it was found to be a potent carcinogen. After stilboestrol was administered to men, it often led to atrophying of their testicles. In other cases, chemical castration was combined with aversion therapy (to be discussed further below). In this case, after men were exposed to same-sex stimuli, they were subjected to negative stimuli, such as electric shocks, drugs that induced nausea, or talk therapy that caused negative thoughts. The idea was to produce a conditioned reflex where homosexual thoughts would be associated with negative outcomes such as pain, fear or discomfort. The combination of chemical castration with aversion therapy turned out to have serious negative consequences. Studies showed that LGBTQ+ individuals subjected to these techniques were almost twice as likely to attempt suicide.
Lobotomy for Gays: Until 1973 homosexuality was considered a mental illness. In the first half of the 20th century, one treatment for homosexuality was a lobotomy. The medical procedure lobotomy was introduced by Egas Moniz in 1935. This procedure severs connections in the brain leading to and from the prefrontal cortex. The procedure is sufficiently barbaric that it is hard to believe Moniz shared the 1949 Nobel Prize for Physiology or Medicine for developing this technique. Although some patients were able to return to work following a lobotomy, many others experienced severe and permanent impairment. Figure II.2 shows lobotomy knives that were used in such procedures.

The most enthusiastic American practitioner of the lobotomy was Dr. Walter Freeman. In the 1940s and 1950s, he performed at least 20,000 lobotomies. In many cases these were performed on patients in hospitals for the insane; but in addition, many lobotomies were performed on homosexuals. Whereas Egas Moniz and his followers tended to sever connections with the prefrontal cortex, Freeman invented a technique called “ice pick lobotomy.” Freeman would take an orbitoclast (an instrument similar to an ice pick, shown in Fig. II.3), insert it next to the eyeball and simply jab at the prefrontal cortex. This was a stunningly crude and brutal procedure. However, Freeman was fond of it because it could be executed extremely rapidly. Freeman would incapacitate patients with an electric shock before performing the operation in about ten minutes; and this “operation” did not need to be performed in a hospital.

The lobotomy was claimed to produce positive outcomes for many patients in mental hospitals. It was especially “effective” with patients who were in severe pain or who cried out incessantly. After the operation, many of them were quiet and placid. However, in many cases this was because the operation had disabled their ability to communicate with others. Norbert Wiener, the inventor of cybernetics, made a telling criticism of lobotomy in 1948. “Prefrontal lobotomy … has recently been having a certain vogue, probably not unconnected with the fact that it makes the custodial care of some patients easier. Let me remark in passing that killing them makes their custodial care still easier.” Doctors in the Soviet Union banned the use of lobotomies in 1950, and they complained that “Through lobotomy an insane person is turned into an idiot.” Over the years, the awarding of the Nobel Prize to Dr. Moniz has been called “an astounding [error] of judgment … a terrible mistake.” We agree with that statement.
Electroconvulsive Therapy:
Electroconvulsive therapy (ECT) is a medical technique where an electric current is passed through the brain. It is still used for some conditions such as major depression or catatonia, but only after all other methods of treatment have failed. Figure II.4 shows equipment used in electroconvulsive therapy.

From the 1950s to the early 1970s, electroconvulsive therapy was used to treat homosexuals. In these cases, the procedure was used more as an instrument of terror, as a form of aversion therapy. The legs or arms of the patient were attached to electrodes. The patient was then shown erotic pictures of same-sex individuals. When they viewed the pictures, the patients were given a significant electric shock. When patients viewed erotic photos of the opposite sex, no shock was administered. Later, the patients were given buttons to control the images they were shown. When shown a photo of the same sex, no shock was given if the subject pushed the button sufficiently quickly.
Needless to say, electric shock procedures had very low rates of success. However, many of the patients reported the persistence of trauma, depression, fear, and possibly post-traumatic stress disorder (PTSD). There were relatively few volunteers for such practices. Many people were referred to these clinics by families, by churches, or by the police if people had been arrested for performing homosexual acts. Once the DSM was changed in 1973 so that homosexuality was no longer listed as a mental disorder, ECT treatment for homosexuals fell out of fashion.
After 1973, medical professionals realized that methods such as castration, chemical castration, lobotomy or electric shock therapy were unnecessary and harmful because homosexuality was no longer considered a mental disorder. There was strong opposition by the medical community towards using these techniques to “cure” homosexuality. Such techniques had terrible physical effects on LGBTQ+ individuals. In addition, we now know that they produced a number of extremely negative psychological effects. To add insult to injury, although in some cases the resulting trauma was sufficient to suppress homosexual behavior, such techniques almost never resulted in a “cure” for same-sex attraction.
Sexual Orientation Change Efforts (SOCE):
Once the medical community changed their focus and removed homosexuality from the list of mental disorders, there was no scientific reason to submit gays to intrusive and unsuccessful methods to produce a “cure” for being gay. Scientific studies showed beyond a doubt that these psychological methods were not only useless, but they produced lasting psychological damage to many people subjected to these practices. In 2021, the American Psychological Association (APA) produced a definitive resolution on Sexual Orientation Change Efforts (SOCE). This described the results of earlier psychological attempts to cure homosexuality, but it also critiqued more recent efforts in that spirit.
There is no longer any legitimate medical reason to pursue psychological methods to “cure” homosexuality. Nevertheless, there are still several groups and organizations that attempt to persuade homosexuals to reject their same-sex orientation because they consider it “sinful” or “unnatural.” The medical community is firmly opposed to those methods (see the research summarized in Section III of this post, and statements by professional organizations in Section IV). Because scientists have documented the lasting harm done by such techniques, a number of states in the U.S. have banned these practices. As of early 2026, 23 states and the District of Columbia have passed laws that prohibit mental health providers from performing “conversion therapy” or SOCE methods.
The SOCE efforts that persist today are in almost all circumstances motivated by religious beliefs. Current practitioners of SOCE efforts often avoid calling their methods “therapy,” because of the unequivocal denunciation of such practices by medical and psychological organizations. But many states that ban these psychological methods allow exemptions for religious groups. Some examples of current efforts to produce effects such as “relational wholeness” in gays are:
- Talk therapy: this generally involves counseling that treats LGBTQ+ identity as a “developmental disorder” that results from childhood trauma. However, since the medical and psychological community rejects this explanation for homosexuality, such efforts need to fly under the radar in states where these practices are banned. The recent Supreme Court decision addressed this type of treatment specifically because it might be protected by First Amendment free speech rights.
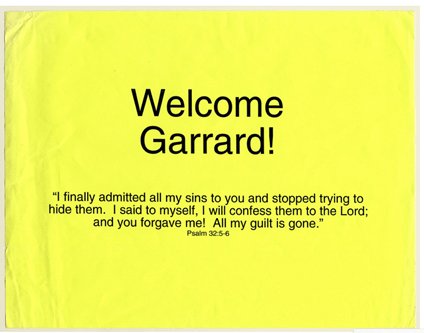
- Spiritual Intervention: This practice is generally carried out through a particular church, where homosexuality is treated as a sin. The intervention may take the form of prayer, healing ceremonies, or counseling with the goal that the individual will “repent” their sin. Occasionally this will involve exorcisms. Figure II.5 shows a workbook entry kept by Garrard Conley, the author of Boy Erased: A Memoir, from a gay-conversion group in Tennessee (now defunct) called Love in Action. Conley’s homosexuality here is treated as a sin, one that Mr. Conley must confess and repent. The APA Resolution on Sexual Orientation in SOCE makes it clear that the damage done in such efforts is no different from that experienced in psychological efforts to “cure” gays.
- Cognitive-Behavioral Framework: These practices claim that same-sex attraction is a form of “addiction” or a “compulsive behavior.” The practices mirror those in treatments of addiction. However, because the medical community firmly rejects the notion that homosexuality is an addiction, people who offer such methods are psychologists who reject the scientific consensus on this issue, and/or they are acting out of religious motivation.
- Aversive Therapy: This is a continuation of methods like electroconvulsive shocks that were administered when subjects were aroused by viewing erotic same-sex materials. However, massive electric shocks would no longer be acceptable. So the continuation of these techniques involves much less drastic techniques than electroconvulsive methods. One aversive technique that is still offered is snapping a patient’s wrist with a rubber band when “unhealthy” attractions are presented.
- Pseudo-Scientific Counseling: This involves a combination of religious belief and psychological counseling. The claim here is that what is being treated are the symptoms of homosexuality. Thus, the individual may be provided with “emotional release” from anxiety, depression or suicidal thoughts. However, the “cure” that is presented involves denying same-sex thoughts and acts and replacing them with heterosexual behavior.
III. RESEARCH ON THE EFFICACY AND DANGERS OF CONVERSION THERAPY
Various forms of conversion therapy are still prevalent today in countries where homosexuality and gender diversity are considered aberrant. Even in the U.S., where LGBTQ+ identities are generally accepted, a 2023 study identified more than 1,300 active conversion therapy practitioners. The majority of patients are homosexual males from conservative religious families who submit themselves or are submitted by their families to therapy intended to eliminate their sinful behavior. A 2020 survey of LBGTQ+ individuals in southern U.S. states found that nearly 8% had been sent to conversion therapy practitioners. Recently, it has become more common for transgender or gender-nonconforming individuals to be subjected to conversion therapy.
The practitioners and supporters of conversion therapy, as well as some independent researchers, have made numerous claims of success in altering patients’ sexual attraction proclivities. In essentially all cases these reports are based on subjects’ self-reporting of the effect of the therapy on their sexual attraction and behavior. The proponents use these reports as “evidence” that sexual orientation is not immutable. These claims are suspect because those who submit to conversion therapy are generally highly motivated to believe that their orientation changes and may therefore either delude themselves or lie about their post-therapy orientation.
The most influential of the claims of success was based on a study carried out in 2003 by Robert Spitzer, published in the journal Archives of Sexual Behavior without normal peer review. Spitzer (Fig. III.1) was a very highly respected psychiatrist and the primary driver of the 1973 DSM change that dropped the designation of homosexuality as a sociopathic personality disturbance. He tried to learn whether people subjected to reparative therapy actually changed their sexual orientation. Reparative therapy is a form of conversion therapy pioneered by psychologist Joseph Nicolosi in which adult patients who seek to change their sexual orientation or gender identity submit to therapy sessions based on a “fusion of spiritual and psychoanalytic thought” with the aim of modifying their sexual behavior (“If gay doesn’t define you, you don’t have to be gay”). Spitzer recruited “200 self-selected individuals (143 males, 57 females) who reported at least some minimal change from homosexual to heterosexual orientation that lasted at least 5 years. They were interviewed by telephone, using a structured interview that assessed same sex attraction, fantasy, yearning, and overt homosexual behavior. On all measures, the year prior to the therapy was compared to the year before the interview. The majority of participants gave reports of change from a predominantly or exclusively homosexual orientation before therapy to a predominantly or exclusively heterosexual orientation in the past year. Reports of complete change were uncommon. Female participants reported significantly more change than did male participants.”
Spitzer’s research design was hardly rigorous. He interviewed only subjects who were committed to change their orientation and relied on their recollections of how they felt years earlier before their reparative therapy had commenced. In the abstract of his paper he admits that “Either some gay men and lesbians, following reparative therapy, actually change their predominantly homosexual orientation to a predominantly heterosexual orientation or some gay men and women construct elaborate self-deceptive narratives (or even lie) in which they claim to have changed their sexual orientation, or both.” In 2003 Spitzer judged those self-reports to be credible. But by 2012 he had reconsidered. He penned an apology to the gay community in which he admitted that “the simple fact is that there was no way to determine if the subject’s accounts of change were valid.”
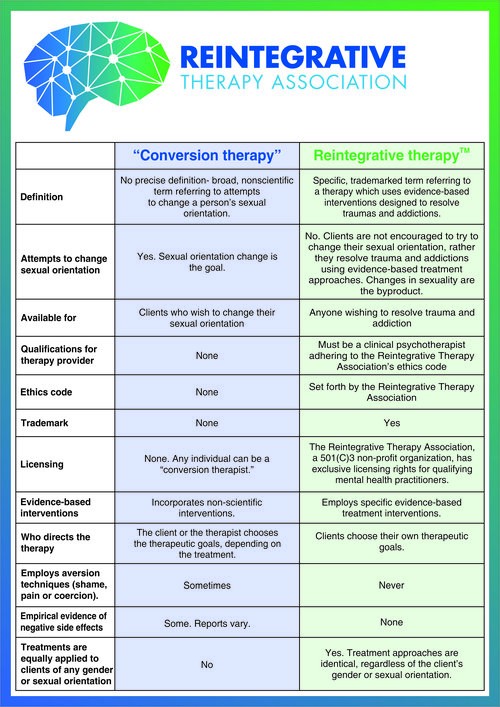
More modern claims of successful conversion, or at least of inducing “sexual attraction fluidity,” remove the reconstructive aspects of Spitzer’s interviews and attempt to quantify change in orientation but still rely on subjects’ self-reporting of questionable reliability. For example, a 2021 study by Pela and Sutton published in the Journal of Human Sexuality – a journal dedicated to the proposition that sexual orientation can be changed through therapy – carried out a longitudinal evaluation over 24 months of 75 adult males who underwent trauma treatment through reintegrative therapy. Reintegrative therapy, developed by Joseph Nicolosi, Jr., “uses established, evidence-based interventions, the same interventions used by other clinics throughout the world to treat trauma and addiction…a female client with binge eating disorder and male client with sexually compulsive behaviors receive the same treatment protocols.” According to Nicolosi, Jr. “As these dynamics are resolved, the client’s sexuality can sometimes change on its own.” Reintegrative therapy works hard to distinguish itself from conversion therapy (for example, see Fig. III.2) but seems to fit well under the heading of cognitive-behavioral frameworks for conversion therapy described in Section II.
Thirty of the originally chosen participants in Pela and Sutton’s study did not complete the therapy protocol. The 75 that did complete the protocol were asked to fill out questionnaires periodically assessing their sense of well-being, their same-sex and opposite-sex experiences and levels of attraction. For example, sexual attraction identity was assessed by the subject’s choice of one among six options first used in assessments by Alfred Kinsey: (1) almost entirely heterosexual; (2) more heterosexual than homosexual; (3) bisexual; (4) more homosexual than heterosexual; (5) almost entirely homosexual; and (6) homosexual. Such choices are inherently subjective because it is not obvious how respondents assess their sexual attraction identity; for example, they may interpret the question to mean their openness to consider relations with either same- or opposite-sex partners, rather than their innate neural and physical response to sexual stimuli.
Questionnaires were recorded at the beginning of the therapy and at six-month intervals thereafter. But only 22 of the 75 participants completed questionnaires after 24 months. The mean results of the questionnaires indicate a shift from an original rating of 4.2 on the above sexual attraction scale to about 3.3. These results demonstrate what a highly selective sample the researchers were working with, without any control group assigned to different forms of therapy. Before therapy the mean response was between bisexual and homosexual, which is the least prevalent orientation among Western males, as seen in Fig. I.1. Furthermore, the participants’ enrollment in the therapy demonstrated their serious desire to suppress their homosexual tendencies. It is neither surprising nor compelling that in such a sample participants would be inclined, on average, to believe that they were a bit more open to heterosexual relations after therapy. And the authors’ suggestion that the effect is lasting is questionable because such a small fraction of the originally chosen participants (22 of 105) actually completed questionnaires out to 24 months. There does not appear to have been an attempt to understand the reasons that 53 of the 75 participants stopped answering the questionnaires. The results are likely to be highly impacted by the self-selection among the continuing participants.
More objective studies of male sexual attraction are possible using methods to assess penile arousal by so-called penile plethysmography (PPG). Most modern applications use penile strain gauges to measure the degree of penile erection when male participants are exposed to videos depicting same-sex or opposite-sex stimuli. The strain gauges are somewhat less sensitive but far less onerous to apply than the technique originally developed by Kurt Freund, which measures air displaced from a chamber placed tightly over men’s genitals. PPG is commonly used in the diagnosis and treatment of erectile dysfunction. Both Freund in 1960 and Conrad and Wincze in 1976 demonstrated that PPG did not support early claims of homosexual men whose sexual adjustment had allegedly been “improved” by conversion therapy treatments.
Unfortunately, since medical and psychological organizations have by now considered conversion therapy to be unethical, ineffective, and potentially harmful, it is unlikely that any Institutional Review Board considering proposals involving human subjects would approve a study designed specifically to test claims of successful conversion by measuring physical arousal of the conversion therapy participants to both same-sex and opposite-sex stimuli, combined with control measurements on homosexual and heterosexual men who have not undergone conversion therapy.
An alternative physical measure of sexual attraction that has been studied recently is pupil dilation in watching sexual stimuli. A 2021 meta-analysis found that “Only heterosexual and gay men demonstrated discrimination in pupillary responses that was clearly in line with their sexual orientation, with greater pupil dilation to female and male stimuli, respectively. Bisexual men showed greater pupil dilation to male stimuli. Although heterosexual women exhibited larger pupils to male stimuli compared to female stimuli, the magnitude of the effect was small and non-significant. Finally, lesbian women displayed greater pupil dilation to male stimuli.” This technique, then, is not sufficiently calibrated to allow reliable assessment of the sexual attraction fluidity claimed by Pela and Sutton.
While we have here considered explicitly only a small fraction of the studies of sexual orientation change efforts, the ones considered are representative. Several task forces have been assembled during this century to review the more complete research literature on both SOCE and GICE efforts. An American Psychological Association (APA) Task Force issued a comprehensive report (see Fig. III.3) in 2009 reviewing the efficacy and risks of change efforts performed up to that date. The APA Task Force concluded: “Given the limited amount of methodologically sound research, claims that recent SOCE is effective are not supported…These [early high-quality] studies show that enduring change to an individual’s sexual orientation is uncommon. The participants in this body of research continued to experience same-sex attractions following SOCE and did not report significant change to other-sex attractions that could be empirically validated, though some showed lessened physiological arousal to sexual stimuli.”
In 2022 Judith Glassgold, who had chaired the 2009 APA Task Force, carried out an updated survey of the SOCE research literature. Her assessment of the reports from 2009 to 2020: “I was unable to identify any methodologically sound studies to evaluate whether SOCE changes sexual orientation… The selection by practitioners or by existing organizations that support change efforts also raised issues of bias in sampling… Claims that SOCE definitively changed sexual orientation in two studies were because of methodological and statistical flaws or unreliable because of methodological limitations.”
The video linked below includes excerpts from a 60 Minutes Australia interview with a former conversion therapist, John Smid, who was involved with Love in Action, one of the largest Christian gay conversion institutions in the U.S., which was renamed as Restoration Path in 2012. But Smid now admits that from his 22 years of experience conversion therapy never succeeds in changing homosexual individuals to heterosexual and in fact does a lot of psychological harm.
In short, there are no objective, quantitative, and reliable tests of successful sexual orientation change or “sexual attraction flexibility” induced by the more modern conversion pretenders such as reparative or reintegrative therapy. Sexual behavior and choice of partners occasionally changes, but there is no evidence that underlying sexual attraction changes. In the absence of reliable indicators of success, condemnations of conversion therapy rely strongly on the indications of potential psychological harm that can be caused by the methods.
Reports of harm induced by SOCE are, of course, also based on subjects’ self-reporting, often based on recollections, but there is less motivation for individuals committed to change their sexual orientation to report harm than there is to report at least partial success. The APA Task Force reported negative side effects of SOCE including “loss of sexual feeling, depression, suicidality, and anxiety. The high dropout rates seen in early treatment studies may also indicate harmful impacts.”
In her 2022 review, Glassgold summarizes research on harm from three influential studies. A 2015 study by Bradshaw, et al. reviewed the impacts of SOCE psychotherapy on members of the Church of Jesus Christ of Latter-Day Saints (LDS). This study found that 37% of the participants found the counseling to be “moderately to severely harmful.” As summarized by Glassgold: “Reported harms included decreased self-esteem, increased self-shame, increased depression and anxiety, the feeling that they had wasted time and money, increased distance from God and their faith institutions, worsening of family relationships, and increased suicidality…Individuals start SOCE with the expectation of change; those who expected a change in sexual orientation perceived greater harms by SOCE. These individuals reported a loss of self-esteem and loss of religious faith.” Some of the participants in Bradshaw’s survey “felt that certain types of SOCE—those conducted by professionals—did provide a forum for discussing psychological conflicts and were more beneficial than religious methods.”
In 2020 Blosnich, et al. used a survey of “a nationally representative sample of 1518 nontransgender sexual minority adults” to examine “how sexual orientation change efforts (SOCE) are associated with suicide morbidity after controlling for adverse childhood experiences.” They found that “SOCE was associated with twice the odds of lifetime suicidal ideation, 75% increased odds of planning to attempt suicide, and 67% increased odds of suicide attempt resulting in moderate or severe injury (the last did not reach statistical significance at p<.05).” In a survey of Canadian sexual minority men Salway, et al. reported in 2020 that among those who had been exposed to SOCE “participants identified both negative mental and physical health effects. The negative mental health effects include suicide attempts and ideation, depression, isolation, and illicit drug use.”
The risk of psychological harm may be even greater when SOCE is performed on children, often at the instigation of families who are distressed about their child’s sexual orientation or gender identity. In a 2020 study of 34,000 sexual minority youth Green, et al. determined the relative risk of suicidality among young LGBTQ individuals who had undergone sexual orientation or gender identity conversion efforts (SOGICE), in comparison with those who did not, “after adjustment for age, race/ethnicity, geography, parents’ use of religion to say negative things about being LGBTQ, sexual orientation, gender identity, discrimination because of sexual orientation or gender identity, and physical threats or harm because of sexual orientation or gender identity.” Their central finding: “Relative to young people who had not experienced SOGICE, those who reported undergoing SOGICE were more than twice as likely to report having attempted suicide and having multiple suicide attempts.”
Ryan, et al. considered the impact on mental health outcomes of young LGBT adults who had been induced by their families to engage with SOGICE. Such youth often see the pressure to undergo SOGICE as family rejection, which exacerbates the mental health risks. The Ryan, et al. study found that “Compared with LGBT-identified young adults who did not receive SOCE, those who did receive efforts delivered by mental health or religious professionals reported serious mental health harms, such as increased suicidal ideation and attempts and depressive symptoms; the rates of these serious mental health conditions were at least 3 times as high among those who received SOCE compared with those who did not… Beyond the negative mental health effects, participants who received a form of SOCE in this study were found to have negative long-term effects such as lowered life satisfaction, less social support, lower socioeconomic status, and other serious difficulties in young adulthood that could affect them over the long term.”
While the APA distinguishes between SOCE and GICE, the same change efforts are generally applied to both aspects of sex and gender identity. A significant difference has been noted by Fish and Russell: “Inasmuch as transgender youths may exhibit behaviors that do not conform with their sex assigned at birth in early childhood, they may be susceptible to experiences of SOGICE earlier in the life course and for longer periods of time. Earlier and prolonged exposures likely have differential effects on later mental health and suicide risk.” Since pre-puberty gender dysphoria occasionally dissipates on its own with passage through puberty, attempts to quantify the success of GICE are even more problematic than for SOCE when the counseling begins before puberty. But surveys do document the heightened mental health risk for children entered into GICE programs.
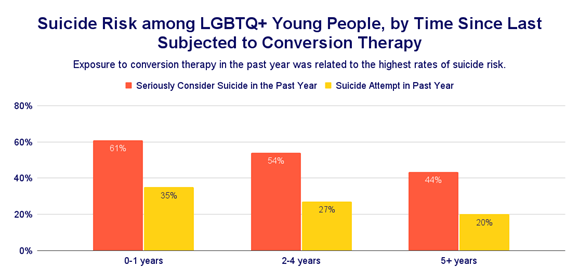
The Trevor Project carried out a 2024 U.S. National Survey on the Mental Health of LGBTQ+ Young People covering more than 18,000 respondents of ages 13-24. The survey revealed that “Transgender and nonbinary young people reported higher rates of conversion therapy compared to their cisgender peers (6% vs 4%).” Of the people subjected to conversion therapy 3% had been exposed before the age of 7, 34% between 7 and 12, 59% between 13 and 18, and 4% between 19 and 24. “The odds of a suicide attempt were lower the older an LGBTQ+ young person was when first subjected to conversion therapy. For each additional year of age at first exposure to conversion therapy, the likelihood of a past-year suicide attempt decreased by 6%.” The Trevor Project found (Fig. III.4) the likelihood of suicidal thoughts or actions was greatest when the exposure to SOGICE was most recent.
Recent research has pointed out that the adverse effects of exposure to conversion therapy may be physical as well as psychological. In their medical evaluations of “703 sexual and gender minority participants aged 16 to 29 years who were assigned male at birth,” Gibb, et al. found the serious cardiovascular issues summarized in Fig. III.5 that showed up among the 10.2% of the cohort who had been exposed to conversion therapy. The effects “remained significant even after the researchers adjusted for behavioral and sociodemographic covariates.”

It is fair to conclude that the harms of SOGICE far outweigh any potential benefits. But individuals with same-sex attractions or gender identity differing from reproductive-organ sex are often under significant minority stress from social discrimination and conflicts with their family and/or religious beliefs. There is thus an important role for affirmative therapy offered by licensed mental health professionals and aimed at helping patients who want assistance to come to terms with their sexuality and gender and resolve the conflicts they may feel about it. The APA Task Force report developed a framework for the appropriate application of affirmative therapeutic interventions based on an understanding that “Same-sex sexual attractions, behavior, and orientations per se are normal and positive variants of human sexuality; in other words, they are not indicators of mental or developmental disorders…[and] Gay men, lesbians, and bisexual individuals can live satisfying lives as well as form stable, committed relationships and families that are equivalent to heterosexual relationships in essential respects.”
Important aspects of affirmative therapy involve understanding all aspects, and particularly religious or spiritual aspects, of an individual’s personal situation, increasing clients’ access to social support, and encouraging active coping strategies that include cognitive, behavioral, or emotional responses to help a client to “resolve, endure, or diminish stressful life experiences.” Research on the effectiveness of affirmative therapy indicates more positive and far less harmful impacts than SOCE. For example, one study found that “those who received affirmative therapy reported fewer symptoms of depression and anxiety following treatment, reduced stress, reduced alcohol abuse, and reduced risk-taking sexual behaviors such as condomless sex compared to the waitlist group.” However, approaches to affirmative therapy are still under development and improvement.
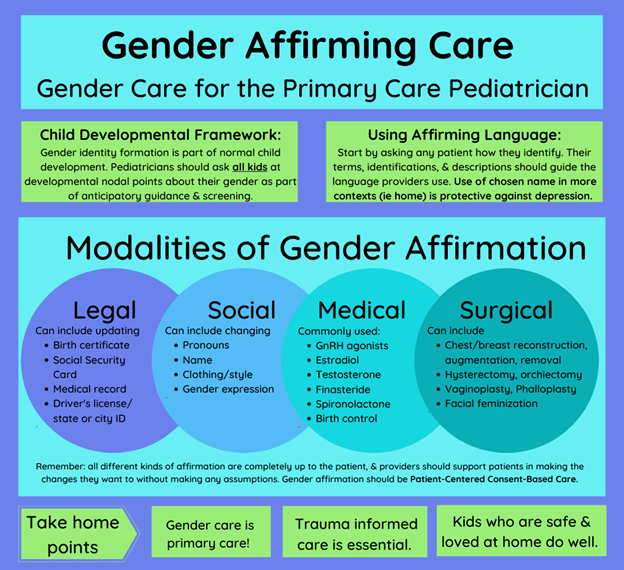
It is important to distinguish between affirmative therapy and gender-affirming care, which in addition to psychotherapeutic care can include legal, social, medical, and surgical interventions, as summarized in Fig. III.6. Among the medical interventions are hormone treatments that aid transitioning.
— Continued in Part II —
