
September 19, 2020
Introduction
The COVID-19 pandemic has spread disease and death around the globe. It has caused an enormous amount of fear and anxiety, because of the spread of the disease and the resulting hardship as entire economies have closed down to “flatten the curve” of cases of the coronavirus. These tensions have been accompanied by a rapid rise in misinformation and intentionally promoted disinformation about the disease and the best ways to combat it. We have previously devoted several blog posts to this phenomenon. First, we published a post on Science Denial and the Coronavirus that covered the period from the first announcement of a new virus until the end of April 2020. We then updated that with a post on COVID resurgence in America. We also produced a post on Dr. Judy Mikovits, an epidemiologist who was the central figure in the viral video Plandemic, and who has championed a number of conspiracy theories. We also published a post on conspiracy theory “true believers,” where we reviewed the psychological characteristics of people who create or support conspiracy theories.
In the United States, misinformation and confusion about the coronavirus pandemic is particularly widespread. There are three main reasons for the spread of false narratives regarding the COVID-19 pandemic.
- The explosion of social media posts about the disease. The increase in societal tension and anxiety creates an atmosphere that is particularly conducive to false information and conspiracy theories. The enormous popularity of social-media sites such as Facebook, Twitter and YouTube means that millions of people are able to share posts, regardless of their veracity. In our post on the QAnon conspiracy theories, we pointed out that Facebook’s algorithms have led people to the QAnon sites (before they were banned by Facebook). People who expressed interest in various political posts would be “steered” by Facebook algorithms to successively more bizarre conspiracy theories, some of them about the pandemic. And the more outrageous the claims made in a post, the more frequently they seem to be shared on social media. Although posts supporting QAnon conspiracy theories are viewed and shared by millions of people, at the same time the central themes of QAnon are also among the least-believed conspiracy theories.
Conspiracy theories regarding the coronavirus pandemic have been widely shared, and have contributed to the confusion and debate over the disease and our response to it. It should also be pointed out that there are active attempts by foreign governments, particularly the Russians, to plant disinformation on social media. These attacks are part of an effort to sow dissent in democratic societies. The coronavirus pandemic has proved to be fertile ground for Russian trolls.
- The Trump Administration, and Donald Trump personally, have been responsible for a great deal of false information about the pandemic. This is in part a result of Donald Trump’s personal characteristics. His clinical narcissism and egotism mean that he invariably tries to portray the image of control, and to foster the notion that his administration is doing a great job. He refuses to read even one-page summaries of briefings, which means that (despite his claim that he is the smartest person in any room) he has very little detailed grasp of any situation. He constantly rewards loyalty rather than competence, so effective staff leave or are fired. Throughout this crisis, Trump has shown a determination to frame situations in a way that he considers most helpful to his re-election campaign.
The results have been entirely predictable. From the first revelations at the end of 2019 about an epidemic of a novel coronavirus until the middle of March 2020, Trump attempted to reassure the American people that the disease was “completely under control” in the U.S., and was nothing to worry about. He did this despite numerous intelligence briefings that the disease posed a real threat to the U.S. We have ended our data survey for this post on September 8, 2020, but on the following day first taped excerpts emerged from Bob Woodward’s new book Rage, based on a series of 18 interviews he conducted with Trump himself. Those excerpts reveal in his own words that Trump understood clearly by early February that the coronavirus was actually deadly and easily transmitted. Nonetheless, he made the gross political miscalculation that his reelection chances would be boosted by “playing down” the severity of the disease enormously – by assuring Americans that it would soon just “disappear” — in order to convey confidence and calm the public and the stock market.
Americans thus received invalid information about the pandemic and personal behavior needed to mitigate its spread on a daily basis from his briefings, starting at an early stage when public opinions were formed and the adoption of suitable strategies could have largely contained community spread. Trump’s own information about the real severity of COVID-19 came in significant part from China, whom he nonetheless continued to blame publicly for failing to contain and share information about the virus. Trump’s actions form a tragic backdrop to the spread of the disease in the U.S., to the many thousands of preventable American deaths, and to the false narratives we address in this post.
Then in mid-March the administration did a sudden about-face and recommended an economic shutdown and several personal guidelines to “flatten the curve.” However, Trump immediately undercut these guidelines by refusing to wear a mask in public and failing to obey recommendations for social distancing. Thus, Americans were treated to a long-running series of false narratives from the White House. For the first eight weeks the narrative claimed that the disease was completely under control and was nothing to worry about. This was followed by the narrative that the federal government was doing a terrific job in managing the pandemic. After much of the U.S. had sheltered in place and locked down their economies, this was followed by the narrative that the country would rapidly rebound and the economy would resume its former vigor. At present we are experiencing the false narrative that the pandemic is essentially over with only “a few embers” remaining, despite the fact that the country is persistently experiencing roughly 40,000 new cases and 1,000 new deaths of COVID-19 every day.
- A third source of the spread of false narratives is the Fox News channel. At present, it acts as a massive propaganda machine for Donald Trump and his administration. A recent book by Brian Stelter discusses in great detail the relationship between Fox News and Donald Trump. With the exception of Chris Wallace and, before he left Fox for CNBC, Shepard Smith, not only do the talking heads on this channel parrot (or plant) the Trump Administration’s narratives, but according to Stelter anchors like Sean Hannity frequently participate with the White House in discussions about Trump policies. This is sufficiently common that it is not always clear where the ideas emanate and who is copying whom. Stelter points out that while most TV news broadcasting begins with a set of facts and follows that with commentary, Fox News primarily focuses on commentary and presents facts “only as an afterthought.” Furthermore, Fox News employs very few reporters; the bulk of their reporting is imported from the Internet, and in particular sites like Breitbart. Finally, Fox News has very few staff who engage in fact-checking or who check content for its veracity.
The net result is that Donald Trump and his administration have what is essentially a large and financially successful propaganda machine. Studies show that people whose main news source is Fox News have strikingly different attitudes and opinions than those who do not rely on this channel. For example, during this pandemic a number of Fox News commentators have singled out Anthony Fauci for criticism; this is because Fauci has been the most outspoken critic of several statements that Trump has made regarding the pandemic. Fox commentators have produced distorted lists of contradictory statements they claim were made by Fauci; more recently, a number of their commentators have adopted the position that “Nobody elected Anthony Fauci, why should we listen to his advice?” (other than the fact that he is probably the most respected epidemiologist in the world?).
Here, we present ten different narratives regarding the COVID-19 pandemic. We discuss each of these at length, tracing their origins and the spread of these ideas. And we provide data that demonstrates why these stories are false. The post is divided into three parts, organized as follows:
Part I:
- False Claim #1: “The coronavirus is a hoax (or perhaps something else entirely)”
- False Claim #2: “The coronavirus is not serious”
- False Claim #3: “No one could have foreseen a global pandemic”
Part II:
- False Claim #4: “No one really knows the best way to deal with the pandemic”
- False Claim #5: “Advice from top U.S. scientists about the coronavirus has consistently been wrong”
- False Claim #6: “The U.S. response to the coronavirus has been ‘the envy of the world,’ particularly with regard to our number of tests”
- False Claim #7: “The mitigations are worse than the disease”
Part III:
- False Claim #8: “The most effective strategy against a pandemic is through the ‘Magic of the Free Market’”
- False Claim #9: “There is already a cure for COVID-19”
- False Claim #10: “Even the development of a vaccine will not stop the pandemic”
- Summary
- References to source material for all three parts
In order that individual False Claims can be perused without necessarily reading straight through the entire post, we have included a small amount of repetition in the different sections.
False Claim #1: “The coronavirus Is a hoax (or perhaps something else entirely)”
As of September 8, 2020, the number of U.S. cases of the Coronavirus is nearly 6.5 million, and the number of American deaths attributed to the virus is over 193,000. One would think that these numbers would convince any objective observer that this COVID-19 pandemic is real and dangerous. However, that is not the case, particularly since there has been an explosion of false information and conspiracy theories on social media. In this post we will divide people who don’t believe the official scientific assessment of this public-health disaster into two categories. The first is people who actually claim that the pandemic is a hoax – that it is not real, or that the SARS-CoV-2 virus is not the cause of illness and death. The second category is those who claim that, although the virus exists, it is not nearly as dangerous and deadly as is claimed by public-health authorities. We will review this second narrative in the next part of this post.
Figure 1.1 shows the world cases and deaths from COVID-19 as a function of time, up to August 6, 2020.
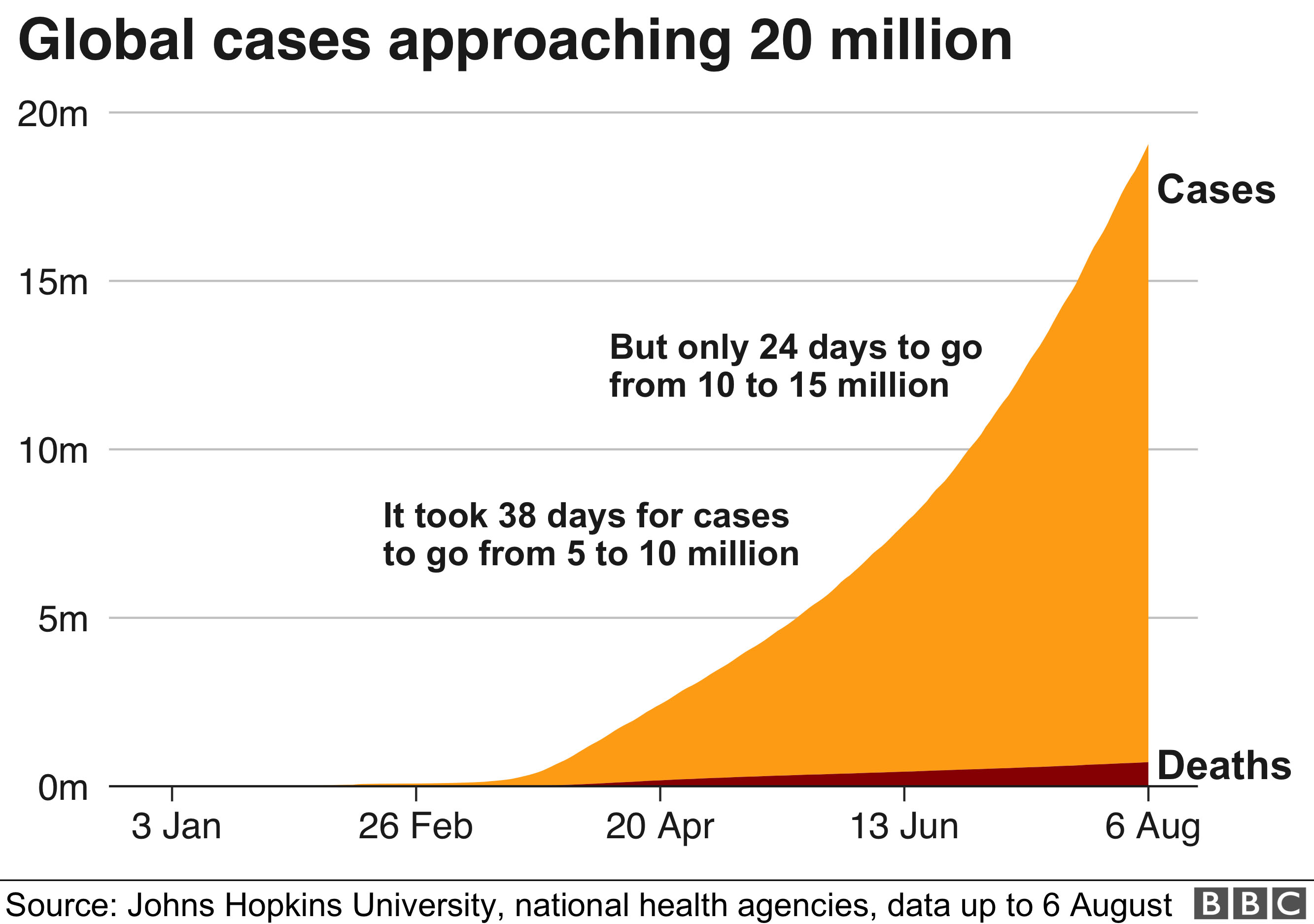
Figure 1.1: World cases and deaths from COVID-19 as a function of time, up to Aug. 6, 2020. From Johns Hopkins University.
Figure 1.2 shows the daily U.S. cases and deaths from COVID-19 vs. time, up to Sept. 1, 2020. The current number of cases and deaths seems to be declining but it could also be reaching a plateau.
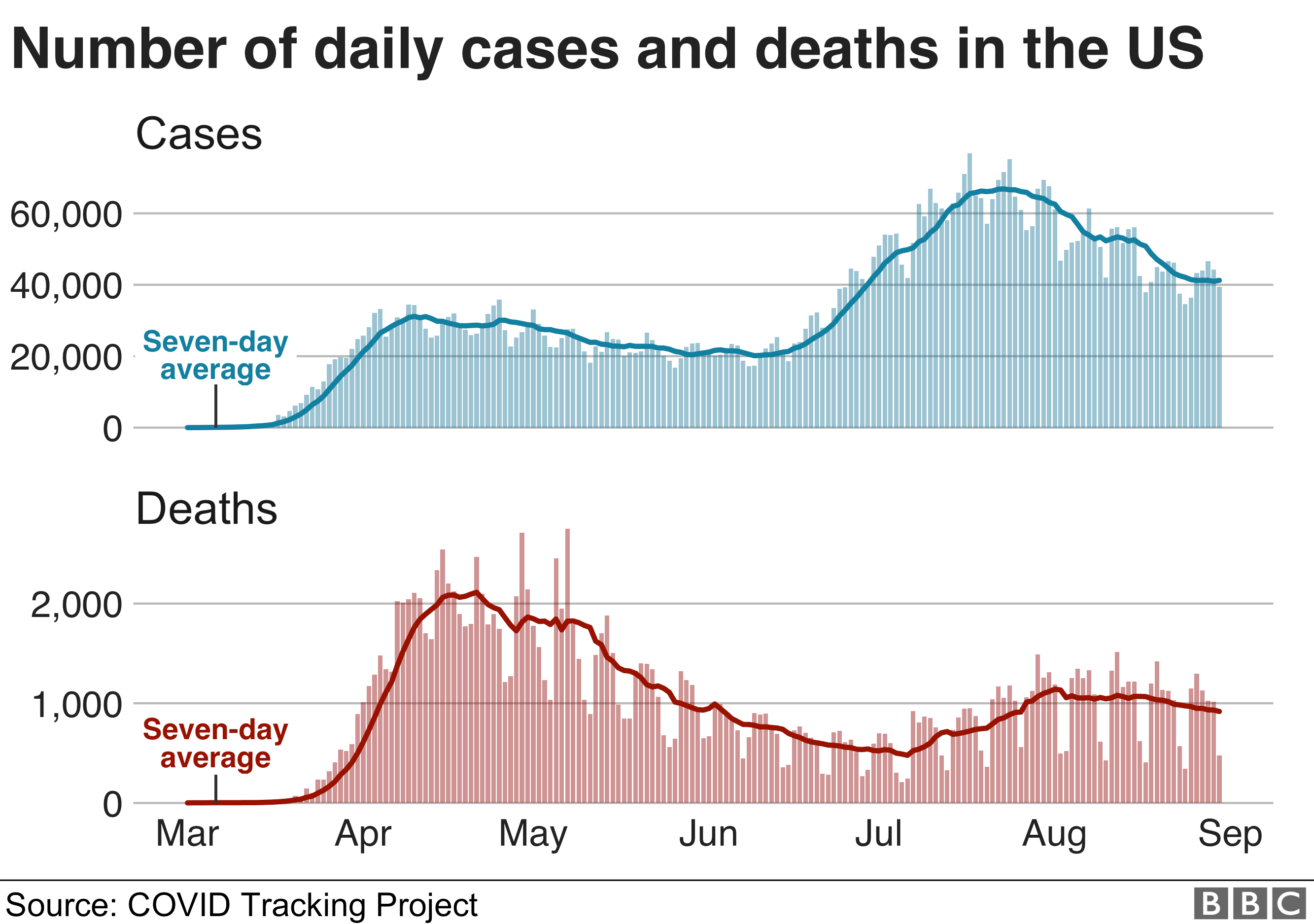
Figure 1.2: US cases and deaths from COVID as a function of time, up to Sept. 1, 2020. Source: Johns Hopkins University.
Early in this epidemic, several people were on record as claiming that the COVID-19 “flu” was either a complete hoax, or else nothing more than the common flu. For example, until the middle of March libertarian Ron Paul was producing posts suggesting that the coronavirus was a “hoax.” According to Paul, governments around the world were simply using this disease as an excuse to take away individual freedoms. “Governments love crises because when the people are fearful they are more willing to give up freedoms for promises that the government will take care of them.” Paul continued, “The chief fearmonger … is Anthony Fauci … Fauci is all over the media, serving up outright falsehoods to stir up even more panic. He testified to Congress that the death rate of the coronavirus is ten times that of the seasonal flu, a claim without any scientific basis.” On his March 16 blog post, Paul concluded “People should ask themselves whether this coronavirus ‘pandemic’ could be a big hoax, with the actual danger of the disease massively exaggerated by those who seek to profit – financially or politically – from the ensuing panic.”
Nowadays, claims that the coronavirus is a complete hoax are limited to fringe regions of the dark Web. But there is at least one other conspiracy-theory claim that the disease is not a virus at all. On January 27, the Web site Connectiv_Events asked the following question: “So what if the deaths weren’t a virus, but a cell breakdown caused by 5G that mimics the effects of a virus?” This post went viral, with people claiming that the COVID-19 pandemic was perhaps not a virus at all, but instead was a set of serious or fatal health effects supposedly caused by the higher electromagnetic (EM) frequencies being used by the new 5G technology.
According to this theory, the new 5G technology produces serious health issues; and corporations backing 5G technology have a vested interest in covering up any side effects, so the “coronavirus” explanation is simply a smokescreen for the harmful effects of this technology. The Website also claimed that “exposure to 5G waves causes flu-like symptoms.” Unfortunately, those claims contradict the statement from an international commission formed by the World Health Organization (WHO). That commission states that “None of the studies on 5G exposure show any conclusive evidence of adverse health effects.”
A related theory speculates that 5G waves cause health issues that make people more susceptible to contracting the virus. Such claims have gone viral (no pun intended) on the Internet. Alexandre Alaphilippe, executive director of the EU DIsinfoLab, a Belgian group that tracks conspiracy theories, says that “Most conspiracies stay online, but this is having real-world impact.” Proponents of the 5G conspiracies fail to deal with the fact that two of the countries that have suffered among the highest per capita COVID-19 death rates, Sweden and Brazil, had no commercial 5G networks implemented this past winter and spring.
For some reason, this particular conspiracy theory was much more widespread in the U.K. and Europe than in the U.S. In Britain, more than 30 acts of arson and vandalism against wireless towers and telecommunications gear took place in the past spring. On April 2 and 3, two wireless towers in the U.K. were set on fire, and a telecommunications box was also set ablaze. It has also been reported that telecom workers have been harassed. Conspiracy theorists also spread rumors that Britain’s shelter-in-place orders were only a smokescreen to allow British workers to install 5G equipment in secret. Figure 1.3 shows graffiti in Britain claiming that 5G is the real cause of the pandemic.

Figure 1.3: Graffiti in the U.K. claiming that 5G is the real cause of the ‘coronavirus’ pandemic.
It did not help that this past January, British Prime Minister Boris Johnson signed an agreement that allowed the Chinese company Huawei to install 5G infrastructure in the U.K. Or that the Chinese city with the largest 5G network was Wuhan. These are just the types of coincidences that are eagerly seized upon by conspiracy theorists. In addition, the Russians have been uploading false claims that 5G signals have been linked to brain cancer, infertility, autism, heart tumors and Alzheimer’s disease. This is part of a much longer-term Russian strategy of spreading malicious rumors in Western democratic societies.
As it happens, the theory that the COVID-19 pandemic is actually a result of the new 5G technology is nearly identical to a theory that developed about the 1889 Russian Flu pandemic. This was a world-wide epidemic that is believed to have originated in Russia in 1889. A very informative article by Alex Knapp in Forbes magazine discusses this pandemic. The Russian Flu subsequently spread across the globe in waves and is believed to have killed about 1 million people. On January 1, 1890, the European edition of the New York Herald ran an article speculating that the cause of the disease might be a novel microbe that was associated with the newly-developed electric light. “’The disease has raged chiefly in towns where the electric light is in common use,’ the article noted, and went on to note that the disease ‘has everywhere attacked telegraph employees.’”
Figure 1.4 shows a fragment of the New York Herald article explicating the theory regarding the origin of the Russian flu.
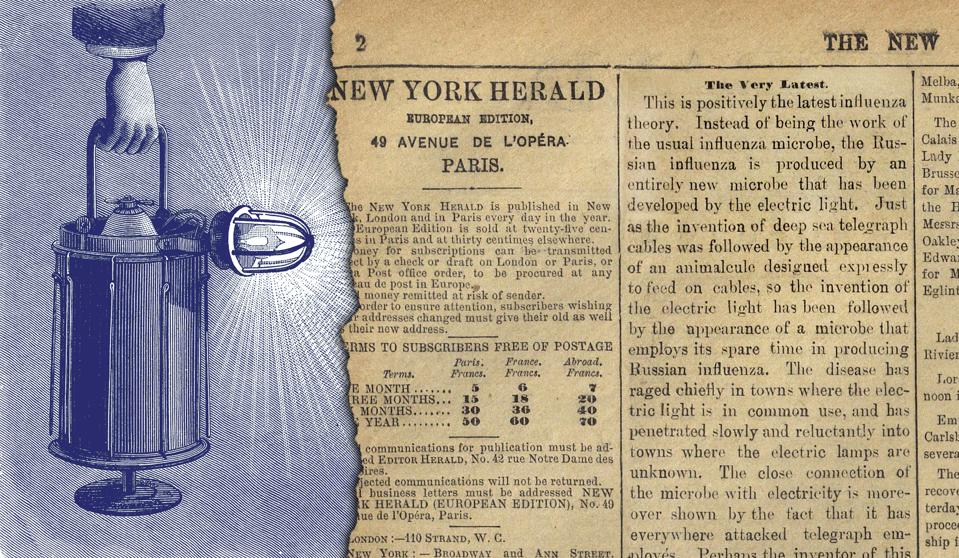
Figure 1.4: The international edition of the New York Herald for Jan. 24, 1890, presenting a theory that the Russian flu is due to a microbe associated with the electric light.
It is worth noting that in 1890, although the germ theory of disease was widely accepted, viruses had still not been discovered. It would be another few decades before it was realized that viruses could cause diseases in humans; and it was not until 1933 that it could be proved that the Russian flu of 1899 and the Spanish flu of 1918 were caused by influenza viruses. In fact, there is now speculation that the Russian flu of 1889 may have been the first coronavirus pandemic. In any case, the scientific situation is vastly different in 2020, when the SARS-CoV-2 virus has been isolated and its genome mapped, revealing several different strains of the virus that help in tracking its spread.
Finally, we will mention two more features of the Russian Flu pandemic that have spooky similarities to COVID-19. First, an 1889 article in The Lancet conceded that “our want of complete knowledge of the nature of the disease renders it difficult to suggest measures of prophylaxis other than the uniform observance of general hygiene rules.” Second, the Russian Flu inspired a number of proposed cures that are now regarded as quack remedies. One drug that was widely (and falsely) touted as preventing the Russian flu was quinine, an anti-malarial drug from which today’s drugs chloroquine and hydroxychloroquine (to be discussed further under False Claim #9 in Part III of this post) have been derived. The more things change, the more they remain the same!
The number of cases and deaths has continued to climb; as of September 8, 2020, there are over 27.6 million cases of the coronavirus and nearly 900,000 deaths worldwide. Thus it is increasingly difficult to allege that the COVID-19 pandemic is actually a hoax. However, there are still very active efforts alleging that this disease is much less serious than is claimed by the public-health establishment. This is the subject of our second false narrative.
False Claim #2: “The coronavirus Is not serious”
Figure 1.2 tracks daily U.S. COVID-19 cases and deaths until about Sept. 1. It now appears that the number of cases and deaths may be decreasing from a second peak experienced in July and August; however, note that on September 1 there are still 40,000 new cases of the coronavirus every day, and 1,000 deaths. So the U.S. is still very much in the midst of a pandemic. And the situation may well worsen again, now that millions of students have returned to schools and colleges, Trump has resumed holding large rallies with closely packed audience members, large non-political gatherings with minimal precautions have occurred in several states, and the spread of virus droplets may be enhanced in cooler, drier Fall weather.
However, Donald Trump and his supporters are eager to act as though the pandemic is over in the U.S. This is associated with his re-election efforts, which currently focus solely on an alleged threat to suburban America from people protesting for social justice. Trump himself almost never mentions the pandemic these days, and right-wing social media echoes his stance by claiming that the COVID-19 pandemic is much less serious than is claimed by public-health officials. We will provide a few examples of this narrative.
Until the middle of March, Donald Trump insisted that in the U.S., the coronavirus was not a problem, and that he and his staff had it “completely under control.” This narrative was supported by pro-Trump commentators like Rush Limbaugh. Early in 2020, Limbaugh ridiculed claims that COVID-19 was a potentially serious epidemic. On Feb. 24, 2020, Limbaugh stated on his radio show “It looks like the coronavirus is being weaponized as yet another element to bring down Donald Trump. Now, I want to tell you the truth about the coronavirus … I’m dead right on this. The coronavirus is the common cold, folks.” On Mar. 13, Limbaugh upped the ante to claim that the coronavirus was actually a hoax. Limbaugh stated “We’re shutting down our country because of the – the cold virus, which is what coronaviruses are. This is COVID-19, the 19th version of the coronavirus. We’re shutting it – can you imagine our enemies watching this? You think the Chinese are not laughing themselves silly over how easy this has been? And it continues.”
In July, Limbaugh complained that many Americans were wearing masks, keeping their children out of school and following the advice of public-health experts. “This isn’t who we are, folks, this cowering and fearful and almost giving up in the face of this enemy … much of the way we are dealing with this is unprecedented – and it’s un-American.” Limbaugh continued by urging Americans to “just deal with it [COVID-19].”
The Fox News channel devotes much of programming by its commentators in amplifying Donald Trump’s messages. They have been leaders in creating and propagating misinformation about the COVID-19 pandemic. They have worked hard to discredit the narrative that the pandemic is serious and deadly, or that the Trump Administration botched the federal response to this disease.
One concerted effort by Fox News commentators is to dispute the scientific consensus on this disease and the reliability of the leading scientific commentators. In this regard, Dr. Anthony Fauci has emerged as the punching-bag for the right wing. Fauci is an epidemiologist who has been Director of the National Institute of Allergy and Infectious Diseases (NIAID) since 1984. During that time he has served under six presidents from both major political parties. He is one of the world’s leading experts on infectious diseases, and he has been a prominent member of the Trump Administration’s Coronavirus Task Force. In that role, Fauci has been widely interviewed by the press and he has presented the scientific consensus of public-health officials and epidemiologists regarding the COVID-19 pandemic.

Figure 2.1: Screen shot of Laura Ingraham on Fox News attacking Anthony Fauci’s comments about the COVID-19 pandemic.
Dr. Fauci has been rather outspoken about the pandemic and the best ways to slow the spread of the disease. In this regard he has frequently contradicted President Trump, whose statements are often governed more by political expediency than scientific accuracy. As a result, right-wing commentators and particularly those from Fox News Channel have focused on criticizing Fauci or accusing him of “changing his story.” For example, in June Laura Ingraham described Dr. Fauci as “the medical Deep State.” When Fauci appeared before Congress, Ingraham reported “Dr. Doom himself at a Senate Hearing today spreading more COVID panic and undermining Trump’s agenda.” As shown in Fig. 2.1, Ingraham then accused Fauci of favoring Joe Biden, saying “Can we all just admit that Fauci is basically working for the Biden campaign?” We will return to criticisms of scientists in False Claim #5 in part II of this post.
A second line of attack is to claim that coronavirus cases and/or deaths have been dramatically over-counted. In April Dr. Scott Jensen, who is also a Republican state senator in Minnesota, stated on Laura Ingraham’s show that the medical community was deliberately inflating the number of cases they ascribed to COVID. Jensen asserted that hospitals were paid $13,000 if they listed the cause of admission of a patient as “COVID-19.” Jensen further stated that hospitals would be paid $39,000 if the patient subsequently went on a respirator. He insinuated that therefore, hospitals were intentionally inflating the number of COVID cases.
Jensen’s statement had a grain of truth to it. Medicare pays hospitals fixed rates for certain conditions; this is based on a system called “diagnosis-related groups,” where Medicare pays a fixed amount to hospitals across the country. Instead of hospitals requesting reimbursement for every Band-Aid and thermometer, they get a fixed rate for every patient with a given condition. The Medicare reimbursement is $13,000 for each COVID patient, rising to $39,000 if the patient ends up on a respirator. However, medical groups and hospitals are adamant that this system does not result in any over-counting. When challenged about his statement, Dr. Jensen denied alleging any misconduct by hospitals as a result of these fees – although, on Laura Ingraham’s show he stated “Nobody can tell me after 35 years of medicine that sometimes these kinds of things impact on what we do.”
Other Trump supporters assert that the number of deaths from COVID-19 is much smaller than has been reported. The most recent example is a post that first appeared on a QAnon site, which was re-tweeted by Donald Trump. The QAnon post retweeted by Trump stated: “This week the CDC quietly updated the COVID number to admit that only 6% of all the 153,504 deaths recorded actually died from COVID. That’s 9,210 deaths. The other 94% had 2 to 3 other serious illnesses and the overwhelming majority were of very advanced age.”
This claim has now gone viral, with many Web sites now contending that less than 10% of deaths attributed to COVID “actually died from COVID;” however, that is a completely false reading of the post from CDC. As part of the information that they mount on their dashboard, the CDC includes information on other conditions, or co-morbidities, for people who have died as a result of COVID. They provide charts that list the numbers of patients who possessed various co-morbidities, which often compromise patients’ ability to fight off the ravaging impacts of the virus. For the week referenced in the claim, the CDC uploaded a chart that “shows the types of health conditions and contributing causes mentioned in conjunction with deaths involving coronavirus disease 2019 (COVID-19). For 6% of the deaths, COVID-19 was the only cause mentioned.” Appearing on Good Morning America, Dr. Anthony Fauci tried to clarify the situation. “That does not mean that someone who has hypertension or diabetes who dies of Covid didn’t die of Covid-19. They did. So the numbers you’ve been hearing — the 180,000-plus deaths — are real deaths from Covid-19. Let [there] not be any confusion about that.” And epidemiologist Gideon Meyerowitz-Katz explained “It’s pretty rare that someone wouldn’t have at least one issue caused by coronavirus prior to their death, and all it means is that in 94% of cases people who had COVID-19 also developed other issues, or had other problems at the same time.”
Figure 2.2 shows part of a table from the CDC report for the third week in August. The chart lists the people who died from COVID during that week. It breaks this down into the number of the deceased with various co-morbidities.
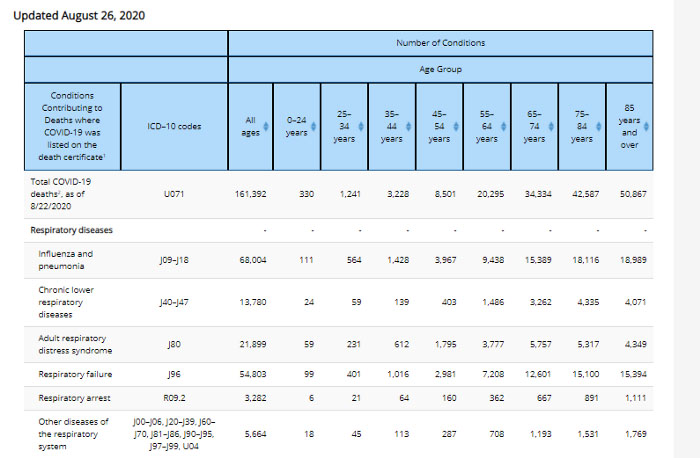
Figure 2.2: Part of a table from the CDC report for the third week of August 2020. The chart lists the number of people with various co-morbidities, who died from COVID during that week.
To reiterate, virtually all of the 180,000-plus deaths in the coronavirus pandemic refer to deaths that were caused by the SARS-CoV-2 virus: the CDC investigated this, and they estimate that at least 95% of deaths attributed to the coronavirus in the U.S. were actually caused by COVID. There are presumably also a significant number of COVID deaths unaccounted for, because the patients die at home without having been tested for the virus. We know that the coronavirus causes other serious conditions such as pneumonia or severe respiratory distress syndrome, two of the most prevalent co-morbidities. In other cases, patients may have pre-existing conditions such as diabetes or hypertension; the presence of these conditions can put patients at higher risk when they develop COVID. There are additional co-morbidities, such as circulatory or renal diseases, that can either be pre-existing conditions or could be caused by COVID.
In all of the cases listed, the patients died as a result of contracting COVID; so the underlying cause of death is listed as COVID. This is exactly the case with patients who contract AIDS and die; the immediate cause of death is frequently pneumonia, however AIDS is the underlying cause for the pneumonia, and AIDS would be listed on the death certificate as the underlying cause of death. The inference that only 6% of deaths attributed to COVID are “really” from the coronavirus is a gross misrepresentation of the truth. Not only did Donald Trump re-tweet this false claim, but he continued to support it in public appearances. In a Sept. 2 interview with Laura Ingraham of Fox News, Trump asserted “’I saw a statistic come out the other day, talking about only 6% of the people actually died from COVID, which is a very interest[ing], that they died for — from other reasons.‘ Ingraham explained that those who die from COVID-19 often have other conditions, but COVID-19 ‘might ultimately have been the key morbidity.‘ ‘But it’s an interesting statistic,’ Trump countered.“
False Claim #3: “No one could have foreseen a global pandemic”
Once his Administration finally acknowledged in mid-March that the coronavirus pandemic was serious and would require drastic steps to control it, Donald Trump repeated several times that COVID-19 was something that could not possibly have been foreseen. On March 26 Trump claimed that “This kind of pandemic ‘Was something nobody thought could happen … Nobody would have ever thought a thing like this could have happened.’” Like many of Trump’s lies, this statement was not only untrue, it was exactly the opposite of the truth.
The fact is that most epidemiologists and many scientists were not only aware that such a pandemic could occur, but they were actively attempting to convince people (scientists, government officials at the state and national level, business leaders and military officials) that a dangerous global pandemic was not only possible but likely. For several years Bill Gates has been thinking seriously about epidemics, as a natural outgrowth of his foundation’s emphasis on public health. In 2015, Gates gave a TED talk called The Next Outbreak? We’re Not Ready. He remarked that Ebola should have been a wake-up call; the world was quite fortunate that Ebola was not transmitted through the air, and that it remained largely in rural areas. However, he stated that a world pandemic, akin to the 1918 Spanish Flu, could have devastating effects, and he emphasized that the U.S. was not prepared for a rapid-spreading epidemic. Here is Bill Gates’ 2015 TED talk:
As you can see, Gates is remarkably prescient in foreseeing the current course of COVID-19. In addition to warning about the deadly effects of a worldwide epidemic, Gates then outlined steps we should take to prepare for a pandemic. The last sentence in Gates’ talk was “If we start now, we can get ready by the next epidemic.” When Donald Trump took office, Bill Gates visited him and once again suggested that the U.S. take advance precautions so the nation would be poised to act quickly in the event of an epidemic. We now see the catastrophic results of the Trump Administration not only disregarding Gates’ advice, but apparently forgetting about his warnings.
Trump also claims that his administration’s response to the pandemic was hampered because of “a broken system we inherited” from past administrations. Once again, this is completely false. Not only did previous administrations realize the probability of a serious epidemic, they underwent extensive planning for such a public health emergency. They ran simulated exercises for hypothetical outbreaks, to test their preparedness for such catastrophes. They collected the results of these simulations in “playbooks” that listed the steps required to contain an outbreak, tabulated those actions that were successful and highlighted the potentially weak links in supply chains and public-health infrastructure.
Dr. James Lawler was a member of the White House National Security Council (NSC) under both George W. Bush and Barack Obama. He stated “I think that this current pandemic has really played out in many ways similar to exercises and table-top simulations that we had done many years ago.” George W. Bush himself said in 2005 “If we wait for a pandemic to appear, it will be too late.” And Tom Bossert, who worked for both the Bush and Trump administrations in homeland security, said “Those strategies and those plans were comprehensive, and they addressed a number of issues that we’ve now seen unfortunately coming to light.”
So how did the U.S. manage to screw up their response to the COVID-19 pandemic? Why did they delay so long in mounting a federal response to this threat, and why did the Trump White House then undercut the plans that had been crafted by their own scientists? As we will see, several of the singular features of the Trump Administration, and of Trump’s own personality, played significant roles in our current crisis.
Here is a timeline of both real-world health crises and epidemic-simulation exercises over the past two decades, as compiled by Maxman and Tollefson:
- 2001: An exercise called Dark Winter simulated a bioterror attack using smallpox; a few months later, a number of American officials were subjected to attacks by letters containing anthrax.
- 2003: Severe acute respiratory syndrome, or SARS, first appears in Asia, and spreads to more than 25 other countries.
- 2005: The World Health Organization (WHO) crafts an agreement through which participating countries will improve and coordinate surveillance and reporting of epidemics.
- 2009: Swine flu (H1N1 influenza) appears in the United States; it causes 575,000 deaths worldwide but less than 13,000 in the U.S.
- 2014: An outbreak of the Ebola virus occurs in West Africa.
- 2015: An outbreak of Zika virus arises in Brazil.
- 2017: The World Economic Forum runs a pandemic simulation at their meeting in Davos, Switzerland.
- 2018: Ebola outbreaks occur in the Democratic Republic of the Congo.
- 2019: Event 201, which simulates a novel coronavirus pandemic, is held in New York City.
- 2019: In December, a novel coronavirus, SARS-CoV-2, breaks out in China. It quickly spreads throughout the world. As of September 6, 2020, more than 27.15 million people worldwide have been infected with over 889,000 deaths worldwide. In the U.S., 6.28 million people have been infected and 189,000 have died.
Even before COVID-19, preparedness for a global epidemic had been a central feature of federal government planning for nearly two decades. In 2005, George W. Bush read a book on the 1918 Spanish Flu pandemic. Struck by the toll from that pandemic and the strains it placed on the public-health system, Bush created a team tasked with planning a coordinated response to a similar outbreak. This planning was given an extra incentive by a 2005 avian flu that had significant impact in Eastern Europe. Dr. Julie Gerberding was the Director of the Centers for Disease Control (CDC) from 2002 to 2009. She describes the plan developed by her office as emphasizing “The importance of testing and diagnostics, the need to stockpile antivirals at the state and national level,” and the necessity to “be able to provide … personal protective equipment.”
Following the 2003 SARS pandemic, the member states of the WHO created a set of rules called the International Health Regulations. These included commitments by countries to invest in pandemic preparedness and to report outbreaks to the WHO. These regulations were utilized in the 2009 H1N1 epidemic, the 2013 Middle East Respiratory Syndrome (MERS) epidemic in 2013, and the Ebola outbreak in 2014-2016 and again in 2018. In 2006, Congress passed the Pandemic and All Hazards Preparedness Act; this included funding for research on emerging diseases and was designed to improve the federal public-health and medical-response capabilities in the event of an emergency.
Shortly after Barack Obama became president in 2009, the U.S. faced the H1N1 swine flu pandemic. While the pandemic accounted for 575,000 deaths worldwide, it caused fewer than 13,000 deaths in the U.S. The CDC credited the Obama Administration’s “complex, multi-faceted and long-term response” for the relatively successful U.S. experience with this epidemic. The CDC also said that federal assistance to states for testing, a robust contact-tracing program, and “quickly, proactively and transparently communicating accurate information to the public and partners” as significant factors in tackling the swine flu.
Before leaving office, the Obama Administration prepared a detailed process that the federal government could undertake to fight global health crises. Obama’s epidemic task force was led by Ron Klain, who directed this effort after it became clear that the U.S. was not prepared for the Ebola epidemic that occurred between 2014 and 2016. According to Klain, the Obama staffers left the report for the Trump Administration when they took office. “It was called ‘Pandemic Playbook’,” said Klain. However, in 2018 while John Bolton was National Security Advisor, it is claimed that “the single office in NSC that focused on biodefense and bio-preparedness” was disbanded. This statement has been challenged by some senior Trump administration officials who allege that the group was simply re-assigned to another office, rather than being disbanded.
A global pandemic was hardly a surprise. Groups of scientists, business leaders, government and Defense Dept. officials regularly ran epidemic simulations, in order to spotlight how disruptive such pandemics can be. The aim was to show “the immense human and economic toll of a global pandemic.” In fact, such a simulation of a global pandemic took place in New York City in October 2019, under the leadership of Ryan Morhard of the World Economic Forum. This was described in a recent article in Nature by Amy Maxman and Jeff Tollefson. Morhard wanted the participants “to confront the potentially immense human and economic toll of a global outbreak.”
In the most serious scenarios studied by such groups, the global toll reached up to 50 million or more deaths, and put the entire global economy “into free fall.” Such scenarios identified the vulnerability of governments to such events, and highlighted the necessity for government and health leaders to be prepared in advance for such health crises. The simulation exercises also showed that it was crucial to spring into action as soon as possible after the onset of a global health crisis.
In 2019 the Global Health Security Index compared governments around the globe in their preparedness for such an emergency. Considering 100 different factors, the group ranked the U.S. #1 in the world in preparedness for such an emergency. So, one would expect that the U.S. should have been extremely well prepared to cope with a pandemic. However, these rankings evidently did not account for the incompetence and dysfunction of the Trump Administration. Maxman and Tollefson ask “Why did dozens of simulations, evaluations and white papers fail to predict or defend against the colossal missteps taken in the world’s wealthiest nation?” Their answer is presaged in the abstract to their article: “Two decades of war-game scenarios foresaw leaky travel bans, a scramble for vaccines and disputes between state and federal leaders. But none predicted Donald Trump.”
The world first learned of the existence of a flu-like epidemic in China at the end of 2019. From the middle of January until the middle of March, President Trump squandered the opportunity to develop a plan to fight the epidemic, while insisting that he personally had the situation firmly under control. Trump apparently felt the need to assert his control over the situation; also, Trump has always viewed the pandemic from its possible effect on his re-election campaign. On January 22, 2020, asked whether he was concerned about the seriousness of the epidemic, Trump responded: “No. Not at all. … It’s one person coming in from China, and we have it under control.” On Feb. 2, in an interview with Fox News host Sean Hannity, Trump claimed, “We pretty much shut it down coming in from China.”
Another toxic feature of the Trump Administration has been its focus on systematically firing or sidelining government professionals. The Reagan Administration was the first to claim that a major problem in our democracy is the size of government, and to assert that big government is necessarily accompanied by waste and over-regulation. However, the Trump Administration’s focus on “draining the swamp” took this idea much more literally. Their notion was that the federal government could do without all of these so-called “experts,” and furthermore that we would be better off having decisions on public health, international relations, and domestic policy made by staff in the Trump White House. Donald Trump’s annual budget recommendations have invariably called for drastic spending cuts on science and research.
The COVID-19 situation was exacerbated by Trump’s conviction that he is the smartest guy in the room, and that his intuition, his “gut” if you will, invariably identifies the best possible solution, even to problems he clearly does not comprehend. This is accompanied by his stubborn refusal to be briefed on issues. Briefing books that previously ran to thick reports were pared back to 10-page synopses, then finally to one-page summaries. Still, Trump rarely read them. Thus, in the period from mid-January to mid-March, when Trump was insisting that the coronavirus was a non-issue and that “everything was under control,” he was briefed repeatedly that the epidemic was spreading world-wide and that this was a serious issue, likely to pose the most severe national security threat of his Presidency.
Trump has also consistently valued loyalty over competence. The net result is a White House staff that spends considerable time boosting the President’s ego, rather than confronting him with unwelcome facts. For example, presidential economic advisor Peter Navarro described his role with Donald Trump: “My function, really, as an economist is to try to provide the underlying analytics that confirm his intuition. And his intuition is always right in these matters.”
On Feb. 25, Nancy Messonier, the Director of the National Center for Immunization and Respiratory Diseases at the U.S. Centers for Disease Control, warned in a White House briefing of the impending community spread of the virus within the U.S., predicting that “Disruption to everyday life might be severe.” What was the reaction to Dr. Messonier’s remarkably accurate statement? Was she praised, or promoted? No: Trump tweeted that the virus “is very much under control.” Furthermore, she was widely criticized for not clearing her statement with the White House before releasing it. It is even reported that Trump wanted to fire Dr. Messonier (her statement was immediately followed by a plunge in the stock market). While she hasn’t been fired, she has not appeared as a CDC spokesperson concerning COVID-19 since her February 25 warning.
On Feb. 10, 2020, Trump claimed that the coronavirus would likely “go away” when the weather became warmer, “probably by April, when the heat comes in.” On Feb. 27, Trump claimed that the virus would be temporary. “It’s going to disappear. One day, it’s like a miracle – it will disappear!” Trump has continued to double down on this claim, as he has consistently been completely wrong on this point. Furthermore, Trump has repeatedly been contradicted by his top medical advisor, Dr. Anthony Fauci, one of the world’s leading experts on infectious diseases. Countering Trump’s claim that the disease would “all disappear,” Fauci said that he “anticipated another outbreak” of COVID-19 in fall 2020. The virus did not go away in April, in fact April and May formed the first major peak in COVID cases in the U.S. (see Figure 1.2). The hot weather of July and August brought with it a second peak in U.S. suffering from the disease. The following YouTube video shows 13 times that Donald Trump has incorrectly claimed that the virus “will go away” (by now, he has made this claim significantly more often than just 13 times).
In mid-March, the Trump White House radically changed its messaging regarding the pandemic. It finally acknowledged that this was a serious disease, and a series of recommendations were released in an attempt to control the spread of the virus. On March 17 Trump stated, “We’re asking everyone to work at home, if possible, postpone unnecessary travel, and limit social gatherings to no more than 10 people.” After pooh-poohing the seriousness of COVID-19 for several weeks, Trump completely flip-flopped regarding the virus. “I’ve always known this is a real, this is a pandemic. I’ve felt it was a pandemic long before it was called a pandemic.”
The federal government did mount some serious, coordinated efforts against the spread of the coronavirus, although they came after the pandemic had entered its exponential growth phase in parts of the U.S. However, the Trump Administration also sent conflicting messages regarding the seriousness of the disease and the appropriate steps to be taken against it. The Coronavirus Task Force was initially directed by Health and Human Services Director Alex Azar; however, after a couple of weeks Azar was replaced by Vice President Mike Pence. During the period March 16 to April 24, the Task Force appeared daily on nationally broadcast briefings. However, the briefings were surreal: much of the time was spent preventing Americans from being told the true threat of the disease and the best ways to protect against it. Because Trump’s re-election was a major driving force in these briefings, the Task Force tended to focus only on positive signals about the pandemic and the nation’s economy, and either glossed over or lied about information considered less helpful to the re-election efforts. During these briefings Trump claimed he had “absolute authority” to dictate policies to the states, but that he took “no responsibility at all” for the consequences of his inaction.
Donald Trump frequently downplayed the seriousness of the virus, and sowed confusion about the best ways to protect against SARS-CoV-2. After some initial uncertainty about the efficacy of mask-wearing for this particular virus, epidemiologists were unanimous by March that wearing masks in public and exercising social distancing were essential to “flattening the curve.” However, Trump announced that he would not personally wear a mask. In numerous public appearances during March through May, Trump was never seen wearing a mask, and he rarely enforced social distancing in public. On June 20, Trump held a big re-election campaign rally in Tulsa, Oklahoma. The indoor rally drew 6,200 people, few of whom were wearing masks or obeying social distancing. One of the Trump supporters present at that rally was black entrepreneur and former candidate for the Republican Presidential nomination Herman Cain. Cain did not wear a mask or observe social distancing; in fact, he was outspoken in his disdain for such measures. Cain subsequently caught the coronavirus and died on July 30. Because of Trump’s refusal to wear a mask or enforce social distancing at his events, these precautions have become politicized. Republicans are significantly less apt to wear masks or practice social distancing; furthermore, several Red-state governors refused to mandate such practices in their states. We will deal further with misinformation spread on social media about mask-wearing under False Claim #7 in Part II of this post.
Figure 3.1 shows the development of polarization regarding the severity of the COVID-19 pandemic. Between mid-March and mid-April, beliefs of Republicans and Democrats diverged rapidly and to differing degrees, depending on whether they lived in cities, suburbs or rural areas.
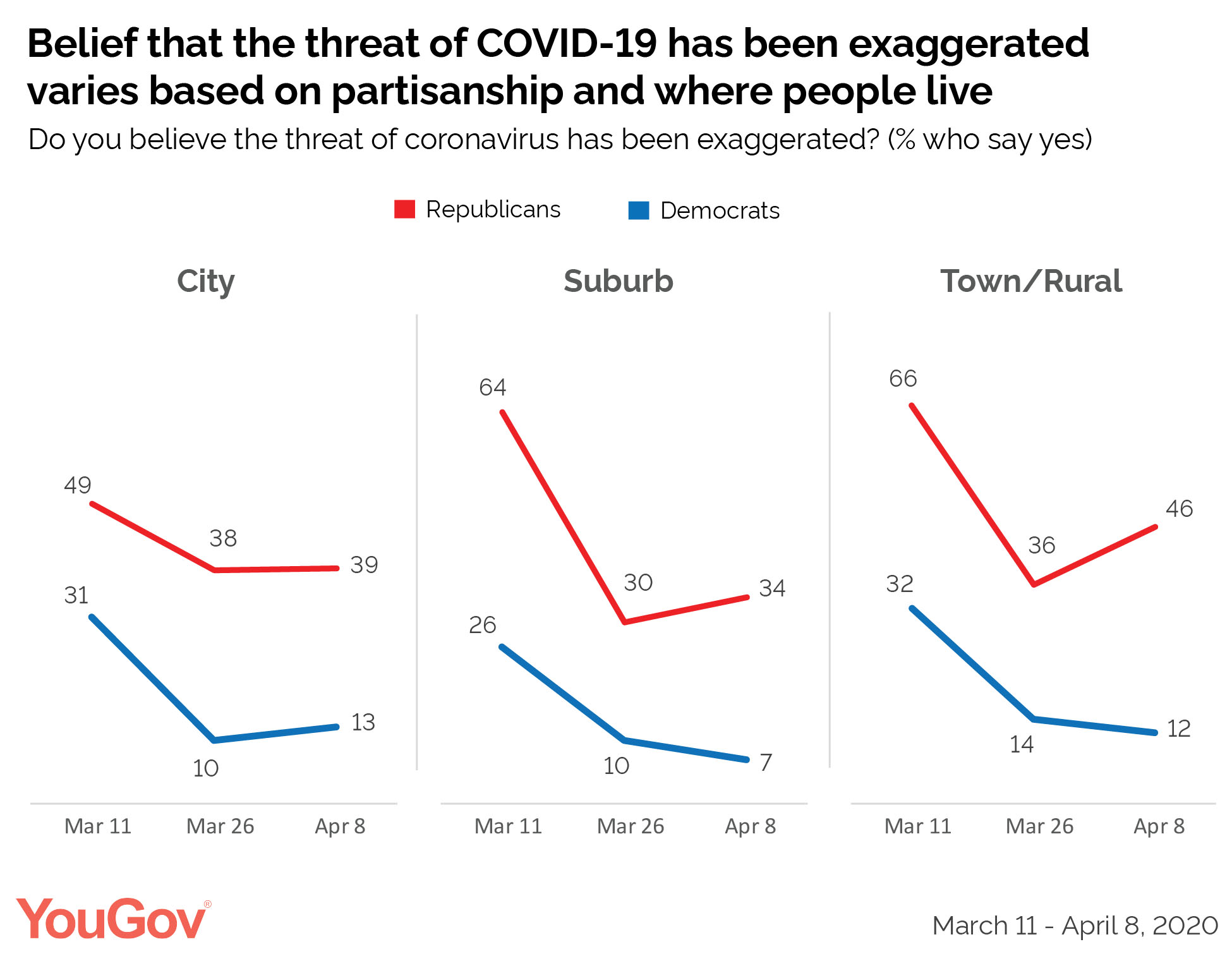
Figure 3.1: Percent of people who believe the severity of the threat from COVID-19 has been exaggerated, depending on where people live and their political affiliation, from March to April 2020.
After the CDC released a set of reasonable guidelines for re-opening the economy, Trump immediately urged states to open up at the earliest possible opportunity. On March 24, just one week after the government advised people to take precautions for 30 days to avoid spreading the virus, Trump claimed that Easter Sunday (April 12) would be a “beautiful time” for people to resume their normal routines. “Wouldn’t it be great to have all the churches full?”, said Trump. “And it’s just about the timeline that I think is right.”
Over the past five months, Trump has repeatedly undercut the advice of public-health officials by urging a speedy re-opening of the economy. On April 14, Anthony Fauci said that “Ultimately, the virus is going to determine when we can safely re-open.” However, the President has contradicted this advice on numerous occasions. In various states, “Re-Open” campaigns were mounted (they were funded by the same groups – the Koch brothers, the Mercer family, and others — that originally bankrolled the Tea Party), and demonstrators claimed that public health directives violated their “liberty.” Many of these demonstrators carried “Trump 2020” signs, and Trump tweeted his approval of their actions. Once again, Trump’s actions confused the public and politicized what should have been bipartisan efforts to slow the spread of the disease.
The net result was an entirely predictable upturn in COVID-19 cases, particularly in the South and West. Some states like Florida and Texas had previously refused to impose mask mandates or restrictions on public gatherings. The state of Georgia re-opened extremely early and allowed establishments such as tattoo and massage parlors to re-open. These states saw massive increases in new cases. However, California, which had imposed significant restrictions at an early period, and which appeared to follow the advice of epidemiologists in its re-opening strategy, also saw dramatic increases in coronavirus cases.
Yet another of Trump’s personal characteristics has exacerbated the spread of the SARS-CoV-2 virus. Trump consistently takes personal credit for everything that has been achieved (or that he claims has been achieved) during his administration, yet he adamantly refuses to take the blame for anything. As a result, once the Coronavirus Task Force had begun plans to secure personal protective equipment and hospital space for COVID victims, Trump announced that the states would be on their own in fighting the pandemic.
A predictable result of this federal hands-off policy was that obtaining supplies became chaotic. States and municipalities found themselves competing with each other and with the federal government for supplies. In the midst of this chaos, on April 2 Trump’s son-in-law Jared Kushner claimed that the purpose of the federal stockpile of public-health materials was “It’s supposed to be our stockpile; it’s not supposed to be state stockpiles that they can then use.” This statement directly contradicted the Website of the Strategic National Stockpile; however, the day after Kushner’s statement, that Website was altered to make its language more compatible with Kushner’s claim.
In similar fashion, Trump has insisted that all K-12 schools re-open for in-person education. He has suggested that the federal government may withhold funds from areas that do not open for all in-person learning. However, the government (and more specifically, the office of Education Secretary Betsy DeVos) have not issued specific guidelines or practices for safely re-opening our schools.
At present, the U.S. has roughly 4.3% of the world’s population, but it has nearly 25% of the world’s COVID-19 cases. The nation is currently experiencing 1,000 or more deaths per day from the virus. This is far more than European countries who had earlier experienced the deadly impact of the pandemic, but who seem to have damped the number of cases, so that their economies have now re-opened and professional sports have resumed. This is shown in Fig. 3.2, which shows the 7-day moving average of new cases in the U.S. and the European Union. While the European case count decreased dramatically after a peak in April, the U.S. count actually increased, despite the fact that U.S. cases lagged behind European ones, which gave the U.S. more time to prepare for a peak in COVID cases.
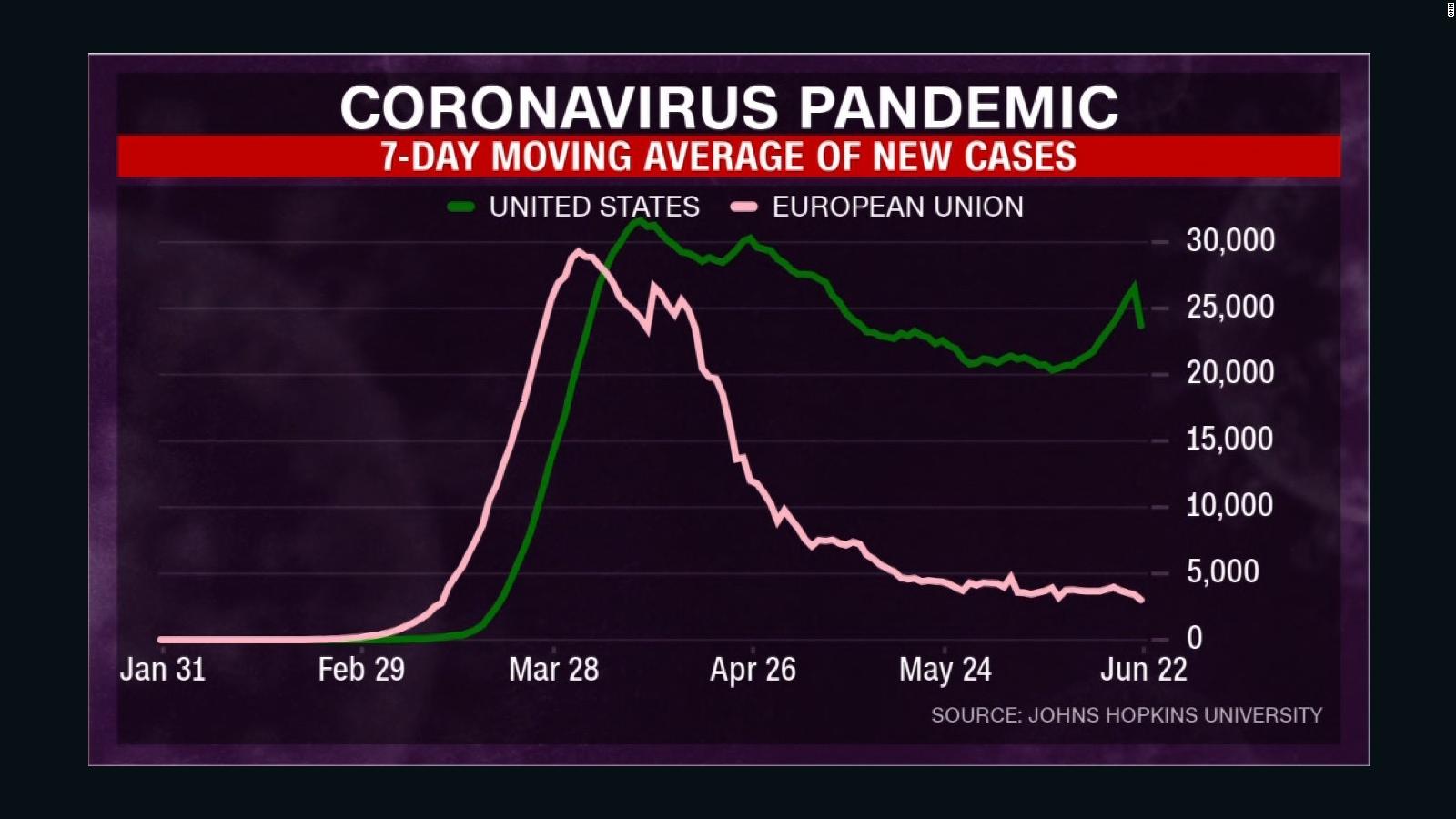
Figure 3.2: 7-day moving average of new COVID cases in the U.S. and the European Union, as a function of time.
In retrospect, the actions of the Trump Administration, and of Donald Trump himself, are responsible for a number of unnecessary American deaths. The title of the Nature article by Maxman and Tollefson reveals the magnitude of the blame assessed to the White House: Two Decades of Pandemic War Games Failed to Account for Donald Trump. It is not easy to calculate the number of unnecessary American deaths in this pandemic; but we will review a few attempts to estimate this number.
The results of pandemic simulations show how essential it is to respond to a public-health crisis at the earliest possible date. On June 19, Isaac Sebenius and James T. Sebenius addressed the following question: Had American leaders taken the decisive, early measures that several other nations took when they had exactly the same information the U.S. did, at exactly the same time in their experience of the novel coronavirus, how many of these Covid-19 deaths could have been prevented?
The Sebeniuses took the following steps. They compared the U.S. response with that of South Korea, Australia, Germany and Singapore. They scaled the population sizes and COVID-19 deaths in those countries to match those of the U.S. And they noted that the pandemic occurred earlier in those countries than the U.S., which gave our government more information to guide their decisions. They applied a “stringency index” developed at Oxford University to measure the speed at which the countries responded, using 14 days from the 15th confirmed COVID-19 case as a comparison date.
The results were as follows. In the four months following the 15th confirmed case, and scaling up each country to produce equal populations, a US-sized Germany would have had 35,049 COVID deaths, compared with 1,758 equivalent deaths in South Korea, 1,324 deaths in Australia, and 1,358 deaths in Singapore. Compared with the 117,858 U.S. deaths in those four months, Sebenius and Sebenius conclude that between 70% and 99% of those American deaths could have been prevented, had the U.S. acted as rapidly as those countries. Results of these simulations should be taken with caution because of uncertainties in the model. However, the results suggest that between 82,000 and 116,000 of those American COVID deaths occurred because of the failure of the Trump Administration to act rapidly, when they first became aware of the epidemic.
The results of this article are in line with other attempts to estimate the number of unnecessary American deaths due to the coronavirus, using different methodologies. An epidemiological model by a Columbia University group simulating the spread of the disease estimated that if the U.S. response had begun two weeks earlier than it did, 80% of the fatalities could have been avoided. And a similar epidemiological model for disease transmission used by Britta Jewell and Nicholas Jewell estimated that up to 90% of the deaths could have been avoided, if lockdowns and social distancing had begun two weeks earlier.
So the truth is that many experts and non-experts did foresee just such a global pandemic. One journalist even presciently predicted, before Trump’s inauguration, that his response to such a pandemic would be highly problematic and feature extensive misinformation. Writing in The Atlantic in December 2016, Ed Yong guessed: “As Donald Trump prepares to become America’s 45th President in January 2017, the question isn’t whether he’ll face a deadly outbreak during his presidency, but when? And more importantly, how will he cope?… If anything, this problem is likely to get worse, given America’s continuing struggle to deal with ‘fake news.’ Inaccurate information can be easily seeded by foreign parties, and given weight and prominence by online algorithms. It’s arguable whether such misinformation made a difference between victory or defeat in the election, but inarguable that it could mean life or death in an outbreak.”
