
January 7, 2021
Introduction:
In recent months, there has been a great deal of discussion about herd immunity. This became a hot topic during the COVID-19 pandemic, particularly the notion of trying to achieve herd immunity in the absence of a vaccine. This idea was driven by several factors. The first was the Trump Administration’s constant pressure to re-open the economy rapidly, even when this contravened the consensus advice of public-health experts. When advice provided to Donald Trump is in opposition to his gut instincts, he casts around for people who will support his positions, and in particular who will support his version of events, even in cases that require creating an alternate set of ‘facts.’ Trump’s conflicts with epidemiologists like Anthony Fauci and Deborah Birx led to the hiring of neuroradiologist Scott Atlas to the White House staff. Atlas had come to prominence during the COVID pandemic for his appearances on Fox News where the Libertarian public-health policies that he espoused dove-tailed nicely with Trump administration priorities. In a similar vein, the publication of the so-called Great Barrington Declaration was widely hailed by Trump and his allies.
In this post, we will discuss the concept of herd immunity and how it is achieved. Next, we will review right-wing challenges to the consensus views of the medical community on how best to combat COVID-19. First, we will discuss the Great Barrington Declaration and its relation to herd immunity. We will review the recommendations of the Great Barrington Declaration and discuss the implications for the public if those recommendations were implemented. After that we will review the public-health recommendations from three libertarian critics, all of whom happen to be Fellows of the conservative Hoover Institution at Stanford University. Spoiler alert: we will conclude that the Great Barrington Declaration recommendations, if they had been implemented in the U.S.A., would have resulted in far higher death tolls, and far more individuals having sustained permanent damage to their health.
Next, we will briefly review the Trump Administration’s disastrous response to the pandemic. We will estimate the number of unnecessary American deaths through the end of 2020. Then we will deal with an argument made by libertarians and anti-vaccination groups, namely that ‘natural immunity’ conferred from infection by COVID is preferable to the immunity provided by a vaccine. Finally, we will review the Swedish experience with the coronavirus. In the early months of the SARS-CoV-2 virus, some right-wing commentators pointed to Sweden as the best way to respond to the pandemic. We will examine whether those recommendations were accurate.
In recent weeks two COVID vaccines, one produced by Pfizer and the other by Moderna, have been granted emergency-use authorization by the Food and Drug Administration. The vaccines are currently being rolled out to the highest-priority candidates before the end of 2020. Once the vaccine is widely distributed to vulnerable groups, this will make many of the arguments covered here moot. However, the policy issues that were discussed here are sufficiently important that we feel it is worthwhile reviewing the arguments for readers. Similar arguments are sure to be re-kindled in the next global public-health crisis. We will also discuss the prospects for achieving herd immunity with the aid of vaccines.
The Concept of Herd Immunity:
Our discussion here follows The History of Herd Immunity, by David Jones and Stefan Helmreich (The Lancet Sept 19, 2020). The concept of herd immunity appears to have originated in the United States in the early part of the 20th century. At that time, the concept was specifically applied to cattle and sheep. Around 1910, there was an epidemic of “contagious abortion,” or spontaneous miscarriages among herds of cattle and sheep. Initially, farmers put down animals that had suffered from this contagious disease. However, in 1916 George Potter and Adolf Eichhorn advocated a novel strategy for fighting this disease, which they termed “herd immunity.” Potter described this concept when applied to herds of cattle. “Abortion disease may be likened to a fire, which, if new fuel is not constantly added, soon dies down. Herd immunity is developed, therefore, by retaining the immune cows, raising the calves, and avoiding the introduction of foreign cattle.”
Potter and Eichhorn proposed to retain the cows that had miscarried. They realized that those cattle would afterwards be immune to this disease. If no new cattle were added to the herd, the fraction of cows with immunity would grow steadily. When the fraction of the herd with immunity reached a certain level, the disease would stop spreading. If the disease occurred again, it would die out rather than spread through the herd. This concept is illustrated in Fig. 1.
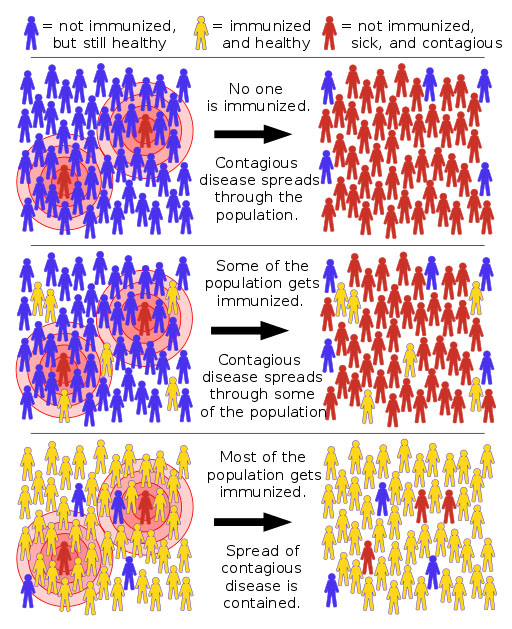
Figure 1: The concept of herd immunity. Upper graph: beginning of pandemic. A few sick individuals (red), with everyone else healthy but not immune (blue). The disease spreads through the community. Middle graph: some of the population is now immune (yellow); the disease spreads but not as rapidly. Bottom: most of the population is immune (the necessary fraction of the population is given by Eq. (1)): herd immunity is achieved. The spread of contagion dies out, no epidemic occurs.
If none of the population has immunity, each sick individual will on average infect R0 other people; this number, called the basic reproduction rate, depends on how contagious the infectious agent is, and the density of the population. The disease will then spread through the community. However, when the fraction of people with immunity (either through having had the disease, or by being vaccinated against the disease) reaches the value F in Eq. (1), the disease will not spread but will die out.
F = 1 – 1/ R0 (1)
This is because at this point, the infected individuals interact mainly with people who have immunity, so that exponential spread of the disease is averted. As the fraction of people with immunity approaches F, the spread of the disease becomes progressively slower.
The idea of Potter and Eichhorn was further extended by W.W.C. Topley. In experiments with colonies of mice, Topley would introduce bacteria that would create an epidemic within the mouse colony. Topley found that as long as he isolated the colony, the epidemic would die out once the number of mice that had been infected, and thus obtained immunity, rose to a certain level. Along with his co-author C.S. Wilson, Topley announced that their mouse colonies had achieved “herd immunity.” Topley then speculated that the insights gained from his experiments with colonies of mice might be relevant to human diseases. He stated that “such a likeness would seem to exist in the case of epidemic diseases affecting children of school age.” And he further suggested that the lessons learned from his experiments might be useful in deciding whether to close schools during epidemics of disease.
The work of Wilson and Topley was applied to epidemics in humans by Sheldon Dudley, who was professor of pathology at the Royal Naval Medical School. Dudley studied young males who were admitted to the Royal Hospital School in Greenwich, England. There, cohorts of students were admitted at regular intervals. They studied and ate together, and slept in large group dormitories. Dudley studied the epidemics of diphtheria that regularly swept through the student groups. He published his results in Proceedings of the Royal Society of Medicine in 1929 in a paper titled Human Adaptation to the Parasitic Environment. Dudley stated that “I will now consider the community, or the herd … Nations may be divided into urban or rural herds. Or we can contrast the shoregoing herd with the sailor herd, or herds dwelling in hospitals can be compared with those who live in mental hospitals.”
Dudley’s use of “herd” to apply to human populations was considered somewhat controversial. The application to human populations of a term more commonly used to refer to animals struck many as having negative connotations. This was particularly the case because the early 1900s represented a high point in the pseudo-science of eugenics in both the U.S. and Britain (see our earlier blog post on eugenics in America). For many people the term “herd” suggested that human communities might be subjected to similar treatments as animal herds, e.g., with respect to populations being manipulated to produce desired characteristics as in the case of animal breeding; or even worse, to undesirable members of the human “herd” being culled. For human populations, the term “community immunity” is increasingly appearing as an alternative to “herd immunity.”
Nevertheless, the concept of “herd immunity” rapidly took hold in scientific circles; and this terminology became even more common once vaccines were developed. At this point, epidemiologists needed quantitative estimates to determine what fraction of the public needed to be vaccinated in order for the society to achieve herd immunity. Let’s consider the case where vaccination confers permanent immunity against a particular disease. We need to determine how infectious the disease is, which will depend among other things on the method of transmission of the disease, and the speed with which the virus spreads among individuals. Let us say that an infected person will, on average, transmit the disease to R0 other people. Then Eq. (1) gives the fraction F of the population that needs to achieve immunity in order to reach the ‘herd immunity’ level. The value of R0 varies greatly according to the disease. This is shown in Fig. 2, which plots the basic reproduction rate R0 vs. the herd immunity threshold (this is the quantity we called F in Eq. (1), expressed in percent).
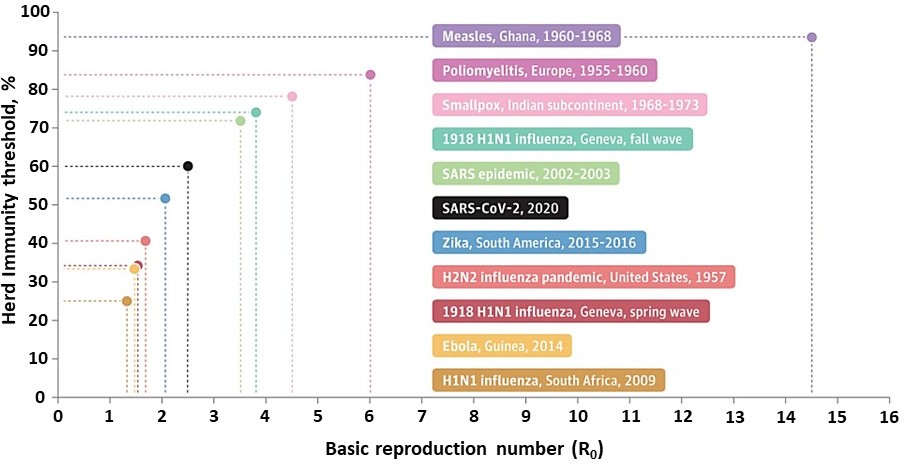
Figure 2: The basic reproduction rate R0 from Eq. (1) vs. the herd immunity threshold F expressed in percent, for several different epidemics, including a number of influenza and coronavirus pandemics, Ebola, Zika, smallpox, polio and measles.
For the coronavirus SARS CoV-2, the virus responsible for the COVID-19 pandemic, Fig. 2 shows that the basic reproduction rate is approximately 2.5. This puts it right in the middle of the various epidemics listed for the past 60 years. The rate R0 varies from a low of about 1.3 for the 2009 H1N1 influenza in South Africa to a high of nearly 15 for a measles epidemic in Ghana in the 1960s. If we assume a value R0 = 2.5 for the coronavirus SARS CoV-2, then Eq. (1) and Fig. 2 show that 60% of the population needs to be immune to the virus, either by having contracted the disease and achieved immunity, or by being vaccinated. Once this fraction F is achieved, then even if the disease is introduced into a population, an epidemic will not occur; the disease may begin to spread but will fairly rapidly die out.
For COVID-19, epidemiologists tend to quote a number of about 70% for the fraction of the population that needs to be vaccinated; this is to insure that those vaccinated exceed the number necessary to achieve herd immunity. In fact, some epidemiologists, such as Anthony Fauci, have recently been recommending increasing F to as much as 85%. The higher value is suggested in order to allow for new, more transmissible variants of the virus as discovered in mid-December, as well as for the highly skewed distribution of reproduction rates about the average R0, suggested by the prevalence of COVID-19 “super-spreader” events where one infected individual transmits the disease to many others. Note that for an extremely infectious disease like the measles, R0 can be as high as 15. From Fig. 2, we see that over 90% of the population needs to have immunity in order to prevent measles epidemics.
Equation (1) is an idealized case that was derived under several assumptions. First, it is assumed that the population density is constant, so that every infected individual comes into contact with roughly the same number of people. Second, it assumes that once a person acquires immunity, that immunity is permanent. Third, it assumes that the infectious agent does not mutate; for a virus, it means that the virus does not evolve into a version which is more highly communicable or for which members of the population no longer have immunity.
If the acquired immunity lasts for only a short time, then it is possible that herd immunity could never be achieved, no matter how many individuals are exposed to the disease or have been vaccinated. This is one of the reasons that you need to get a flu shot every year; the immunity conferred by vaccination is temporary. In addition, the virus that causes the flu is constantly changing. Every year in the Northern Hemisphere a new flu vaccine will be created. It takes several months to produce a new flu vaccine and to manufacture it in sufficient quantities to provide shots for a large fraction of the population. So epidemiologists need to guess what strain of the flu will be dominant several months in the future. They generally assume that the strain of flu most prevalent in the Southern Hemisphere winter (our summer) will be the same one that we experience in the Northern Hemisphere six months later. Vaccines are created that are effective against that strain of flu, and massive quantities of the vaccines are distributed to the population.
In years when the vaccines are very effective against the dominant strain of flu, the number of flu cases can be greatly reduced by vaccination. However, in some years either the flu virus mutates to a form against which the vaccine is less effective, or a different strain of flu appears in the Northern Hemisphere. In those years, the flu vaccine may be much less effective, and the number of flu cases and deaths may rise dramatically.
In the U.S., the population density varies widely across the country; therefore, Eq. (1) would have to be modified to take into account much different population densities in, say, Montana and New York City. Furthermore, the current SARS CoV-2 virus that is causing the current pandemic produces many “asymptomatic” cases, where the carrier may never know that they are infected. And finally, the current pandemic seems to be characterized by a number of “super-spreader” events, where the rate of infection is much higher than average. All of these conditions would modify the herd immunity formula of Eq. (1). Nevertheless, Eq. (1) will still give a rough approximation of the fraction of the population needed to achieve herd immunity.
For our estimates for COVID-19, we will use the value R0 = 2.5, and we will assume an average death rate going forward of 0.6% among infected individuals — these seem to be reasonable guesses, although it must be noted that deaths from COVID-19 vary dramatically according to age; people over 70 with compromised immune systems are in the highest-risk category, while young children seem to have very low death rates. With an average COVID-19 death rate of 0.6%, in the absence of a vaccine and without proven treatments for the virus, approximately 200 million Americans would need to contract the coronavirus before herd immunity could be achieved; and of that group, about 1.2 million people would die. Furthermore, if the antibodies from the coronavirus are effective only for a short duration, then many more people would die before herd immunity was achieved; as we have mentioned, if immunity was sufficiently short-lived herd immunity might never be achieved. Thus, for the coronavirus pandemic the goal of achieving herd immunity before a vaccine is available would require unacceptably large numbers of infected individuals and deaths from the coronavirus; this is the reason that so few epidemiologists recommend trying to achieve ‘natural’ herd immunity for this pandemic.
Challenges to the Medical Consensus on the Coronavirus:
The pandemic has caused nations to make difficult choices between economic shutdowns as a measure to slow the spread of the virus in the absence of a vaccine, and leaving businesses largely open in the hope that individual choices might mitigate the number of cases and deaths from the SARS-CoV-2 virus. There have been several instances where the advice of public-health officials has been contrary to the policies of the Trump Administration. Various groups have taken sides in this debate, and opinions have been divided according to political preferences. Democrats have generally sided with the opinions of scientists, while Republicans have been loyal to administration policies. As we have pointed out elsewhere on this site, Fox News plays the role of cheerleaders for President Trump; several of the most-watched Fox News commentators not only vocally support Trump’s policies, but in some cases it appears that they actually make policy suggestions to the president.
Here we will discuss organized efforts of scientists and political commentators to counter the scientific consensus on the most effective ways to combat the spread of COVID-19. First, we will review the so-called Great Barrington Declaration. This was a set of policy recommendations for dealing with the pandemic. It was issued by scientists with connections to an institute funded by right-wing money. We will review those recommendations and the likely effect on the pandemic if they were adopted. Next, we will review the predictions and recommendations by three senior Fellows at the Hoover Institution. In both cases, we will show that these recommendations better reflect the Libertarian political affiliations of the advocates than reasonable reactions to a public-health crisis.
The Great Barrington Declaration:
The Great Barrington Declaration was a document drafted at a meeting of the right-wing American Institute for Economic Research in Great Barrington, Massachusetts. The document was prepared and signed on October 4, 2020. Note that although the document contains a number of policy recommendations, it was never submitted to peer review or published in a scientific journal. It is just what it states: a declaration. Figure 3 shows a web page where the Great Barrington Declaration is displayed.
Figure 3: The front page of a Web site that displays the so-called Great Barrington Declaration.
The main authors of the Great Barrington Declaration were Sunetra Gupta of Oxford University, Jay Bhattacharya of Stanford University, and Martin Kulldorff of Harvard University. The American Institute for Economic Research is a think-tank that has received significant funding from the Koch Brothers and other right-wing donors. Figure 4 shows the main authors of the Great Barrington Declaration.
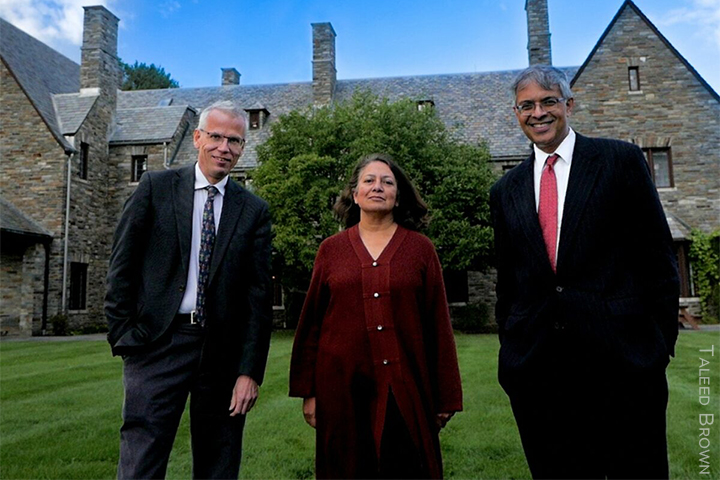
Figure 4: Main authors of the Great Barrington Declaration. From L: Martin Kulldorff; Sunetra Gupta; Jay Bhattacharya.
The document notes that the risks of dying from COVID-19 vary dramatically with age; older people face a much higher risk of death, whereas children face much lower risk of death or serious injury. Furthermore, the risk of death from COVID can be greatly increased if the individual has risk factors such as respiratory illness, heart disease, or diabetes; and the risk is also greater for people with obesity. The Great Barrington Declaration proposes that people in lower-risk categories, particularly children, be allowed to resume their normal lives, while higher-risk individuals should be “shielded” from infected individuals. The authors call for an end to any mandatory restrictions on individual activities; in particular, they oppose any mandatory stay-at-home orders on a population, or shutdowns of certain classes of business.
The Great Barrington proposal signatories favored a return to “life as normal” even without a vaccine. They proposed leaving businesses open, and with all K-12 schools and colleges having in-person instruction. It recommended that offices and restaurants remain open, and also that mass cultural and social gatherings such as churches and athletic activities should have no restrictions on participants. In particular, establishments such as restaurants, bars, gyms and massage parlors, that appear to be especially prone to spreading the disease, would remain open if the Great Barrington Declaration proposals were adopted. Businesses would not shut down, and individuals would decide whether they wished to patronize these businesses.
The authors of this document state that those individuals at high risk from the coronavirus should be “shielded” from the remainder of the population. However, in restricting the length of this document to a single page, so that it be easy to read and have the maximum possible impact, the authors provide absolutely no details on how this “shielding” would take place. How, for example, would the seniors in nursing homes be shielded from the younger staff who provide services for them, if those staff members were told they needn’t follow significant social distancing measures? The proponents of the Great Barrington Declaration claim that their proposal would have great benefits for poor people, in that they could send their children to schools rather than trying to care for them at home. However, the poor are also the least able to maintain social distancing between children and seniors, and thus are likely to be most susceptible to being infected by children and young adults in their social environment. Furthermore, this declaration does not acknowledge the striking differences between black and brown communities and whites in contracting COVID. The declaration is also notable in that it makes no mention of personal actions to minimize the spread of the coronavirus — in particular, wearing face masks, maintaining social distancing, or widespread testing and tracing.
The Great Barrington Declaration is consistent with libertarian arguments that the economy should generally remain open, and that individuals should decide freely what actions they would take regarding the pandemic. Libertarians are in favor of extremely limited government. They view all centralized government with suspicion, so it is not surprising that they oppose restrictions on individual liberties, even as temporary mitigating measures in the face of a pandemic. The pandemic has seen protests by several groups against any required mitigations to limit spread of the coronavirus. In many cases, right-wing activists have claimed that even temporary public-health restrictions on individual actions or choices violate the “liberty” of Americans.
On this point the activists seem to be naïve. Americans do not have the “liberty” not to buckle their automobile seatbelt, or to smoke in public places, or to shout “fire” in a crowded theater. In his book Four Essays on Liberty, philosopher Isaiah Berlin said that “Freedom for the wolves has often meant death to the sheep.” That is, ‘liberty’ for individuals can be constrained when such actions infringe on the well-being, or even the life, of other individuals. Surely temporary restrictions on freedom of movement or assembly are justified in a public-health crisis, when violations of those restrictions could infect and kill others?
The Great Barrington Declaration also sets up a false dichotomy when they claim that the choice is between a complete lockdown of the entire economy, and the laissez-faire approach where the entire economy is allowed to return to a pre-pandemic form and individuals choose how they would participate. Almost no one advocates a complete economic shutdown; even in the “lockdowns” in many countries, essential businesses were left open. There are several success stories where countries have imposed a short but wide-ranging lockdown, followed by a staged re-opening of various aspects of the society. Furthermore, the choice is not between a lockdown that leads to disastrous economic consequences, or letting businesses remain open. Countries like Japan, Vietnam and New Zealand have had lockdowns of short duration followed by staged re-openings; in those countries this approach has allowed the economy to rebound faster than countries with no lockdowns. Successful countries have managed to achieve very low numbers of COVID deaths with relatively robust re-opening of the economy. The U.S. is an example of a country where rapid re-opening of the economy and failure to comply with public-health measures such as wearing a mask and social distancing have led to very high infection and death rates. The resulting rapid spread of the coronavirus has led to situations where officials were forced to re-institute shutdowns to prevent front-line medical workers from being overwhelmed with cases, hospital admissions and deaths.
The authors of the Great Barrington Declaration have been quite vocal throughout the pandemic. In March 2020, Prof. Gupta of Oxford released a widely criticized modelling study suggesting, in one of its scenarios, that half the population of the United Kingdom might already have been infected with COVID-19. In Sept. 2020, she released a pre-print study which argued herd immunity thresholds might be lower than expected due to pre-existing immunity in the population. Those papers, which were not peer-reviewed, have been widely criticized and appear to be highly inaccurate. In September, Dr. Gupta also co-authored a letter to Boris Johnson that recommended a “shielding” strategy for vulnerable populations, rather than the lockdowns that were being imposed by the British government. The letter argued “let’s just do this for the three months that it takes for the pathogen to sweep through the population.” She further urged less vulnerable members of the population “to get out there and get infected and build up herd immunity.”
Dr. Jay Bhattacharya was lead author on a serology study released in April which suggested that as many as 80,000 residents of Santa Clara County, California might already have been infected. Both the methods and the conclusions of that study have been widely criticized.
The authors of the Great Barrington Declaration have called for actions that would involve massive infection of the less vulnerable members of the population. The goal was clearly to achieve herd immunity by exposing a large fraction of the population to the coronavirus. Note that the authors also suggest that herd immunity is much easier to achieve than is generally thought. Their models (which were widely criticized by the epidemiological community) suggested that a vast fraction of the population had already developed immunity to COVID-19. They also suggested that the fraction of the population needed to achieve herd immunity was much lower than the roughly 60% shown in Fig. 2 and suggested by Eq. (1). As we mentioned earlier, Eq. (1) is simply a crude approximation, and more sophisticated models may obtain a lower number or, more likely, a higher number. However, some of the Great Barrington authors and others suggest that herd immunity might be obtained when as little as 10% of the population have been infected. Furthermore, these authors and other COVID skeptics suggest that a large fraction of the American population may be protected against adverse effects from COVID because their bodies already contain T-cells capable of fighting off the coronavirus.
A Stanford University study released on Sept 28 2020, found that about 9% of the U.S. population had been infected with the coronavirus. The findings of this study were based on a national analysis of antibody levels from patients on dialysis in July 2020. The research group analyzed blood samples from more than 28,000 patients undergoing dialysis in 46 states. Dr. Julie Parsonnet, a lead author on the study, said “This is the largest study to date to confirm that we are nowhere near herd immunity.” Note that the findings of this study completely contradict the claims of the Great Barrington Declaration that a very large fraction of the American population might already possess antibodies against the SARS CoV-2 virus.
The Great Barrington Declaration was widely publicized, and it became extremely controversial. On one hand, a large number of people signed onto petitions indicating their support for the recommendations in the declaration. In a couple of weeks, over 175,000 people had signed these petitions. However, it has been noted by the media that a number of the petition signatories were “homeopaths, physiotherapists, massage therapists, and other non-relevant people.” In addition, there were some obviously fake names in the petitions – my personal favorites were Dr. Johnny Fartpants and Prof. Notaf Uckingclue. Nevertheless, the number of signatories was evidence of a significant level of support, and represents even more politicization of the COVID debate.
The response from the international community of epidemiologists was almost unanimously negative. The Director-General of the World Health Organization Tedros Ghebreyesus said that the proposal to let the virus spread in order to obtain herd immunity was “unethical.” He pointed out that “Never in the history of public health has herd immunity [via natural infections] been used as a strategy for responding to an outbreak, let alone a pandemic.”
Dr. Anthony Fauci, the Director of the National Institute of Allergy and Infectious Diseases called the declaration “very dangerous.” He said that “This idea that we have the power to protect the vulnerable is total nonsense because history has shown that that’s not the case … Anybody who has any experience in epidemiology and infectious diseases will tell you that is risky, and you’ll end up with many more infections of vulnerable people, which will lead to hospitalizations and deaths.”
The 12,000-member Infectious Diseases Society of America stated that the Great Barrington Declaration’s proposals were “inappropriate, irresponsible and ill-informed”. And a consortium of American public-health groups published a statement warning that following the recommendations of the Great Barrington Declaration would “haphazardly and unnecessarily sacrifice lives … The declaration is not a strategy, it is a political statement. It ignores sound public health expertise. It preys on a frustrated populace. Instead of selling false hope that will predictably backfire, we must focus on how to manage this pandemic in a safe, responsible, and equitable way.”
We agree with the preceding statement. The authors of the Great Barrington Declaration are letting their medical judgment be over-ruled by their political leanings. This document is the product of people who minimize the seriousness of the pandemic. They believe that individual choices should override public-health recommendations. One interesting thing is that the authors of this declaration deny that they are in favor of trying to achieve herd immunity. However, herd immunity is clearly the goal of this strategy; and both the Great Barrington authors and the Hoover Institution Fellows who are profiled in the next section have advocated policies that rely on herd immunity through natural infections.
The Hoover Institution Strikes Out:
The coronavirus pandemic has highlighted some serious weaknesses in Libertarian philosophy. Many libertarians maintain that the only legitimate function for a central government is national defense. All other functions, they say, are better handled by states, local governments, or even by individuals acting in their own self-interest. So a national disaster, the type of issue that is often handled best by an effective central government, presents a challenge to Libertarians. And a global issue, that appears to require a coordinated world-wide response, is nearly unthinkable to a Libertarian.
So how have Libertarians responded to the COVID-19 pandemic? Many of them initially dismissed this epidemic as a hoax. Former Texas congressman Ron Paul repeatedly called the pandemic a “hoax” in the early days of the disease. And on Feb 24, 2020 Rush Limbaugh reassured his listening audience “The coronavirus is the common cold, folks.” This nonsensical argument is still heard in some conservative circles today. As the number of cases and deaths expanded in exponential fashion, Libertarians modified their arguments. First, they claimed that the virus was far less deadly than had been claimed. At one point, Donald Trump said that for many people, the disease was “no more than the sniffles,” and that “almost no one” dies from the disease. On Oct. 30, Donald Trump Jr. claimed that the number of Americans dying from the pandemic was “almost nothing” (roughly 1,000 Americans died from COVID-19 that day).
On December 29, 2020, the number of Americans dying from the pandemic is about 3,000 per day. That is equivalent to the number of American deaths from the “9/11” terrorist attacks every day. Nearly 340,000 Americans have died from COVID-19 – this is one out of every thousand Americans. There have been nearly 20 million cases of COVID-19 among the American population. Figure 5 shows the number of daily cases of COVID vs. time since the start of the pandemic up to Dec. 27, 2020. You can see that the number of daily cases in the U.S. is the highest it has been since the beginning of the pandemic. Figure 6 shows the number of daily deaths in the U.S. from the pandemic. It shows that the current number is over 2,500 per day. And Fig. 7 shows the total number of U.S. deaths from the pandemic. Donald Trump keeps repeating that COVID “is going to disappear” – as is evident, at the end of Dec. 2020 the number of COVID deaths is still rising rapidly, and experts suspect that after Christmas there will be yet another “spike” in the death rate. One fear is that Americans are tired of the public-health restrictions and that they may relax now that a vaccine is being distributed. Clearly it will take time until the spread of the disease is curbed.
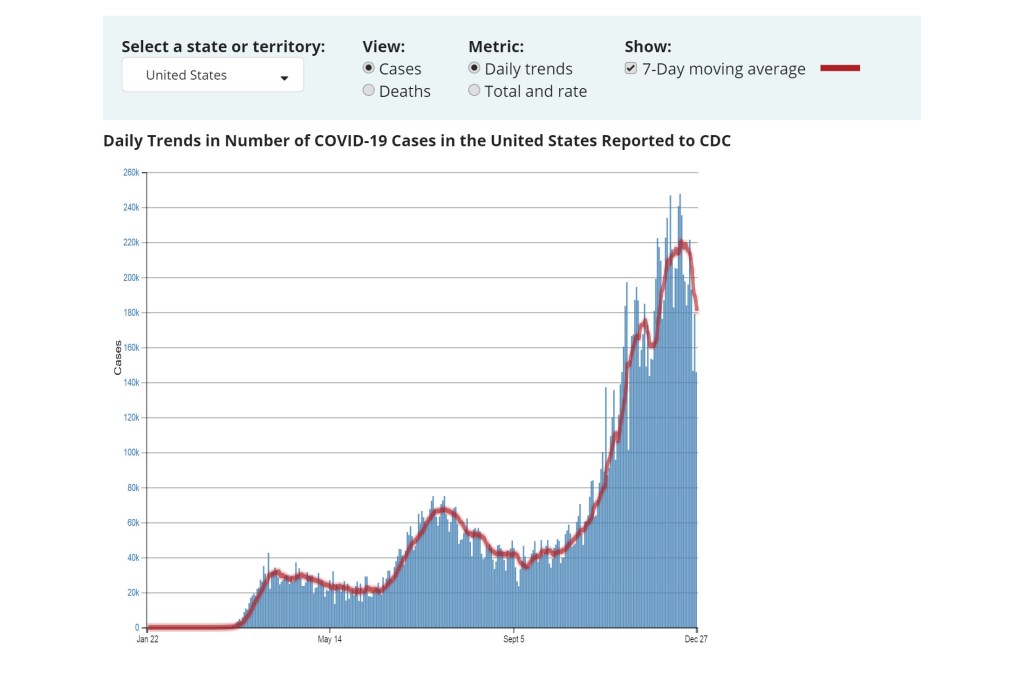
Figure 5: The number of daily cases in the U.S. from the COVID pandemic, vs. time, up to Dec. 27, 2020. The number of daily cases is as high as it has ever been since the start of the epidemic. The post-Thanksgiving peak is passing but a post-Christmas peak may be forthcoming. From the CDC.
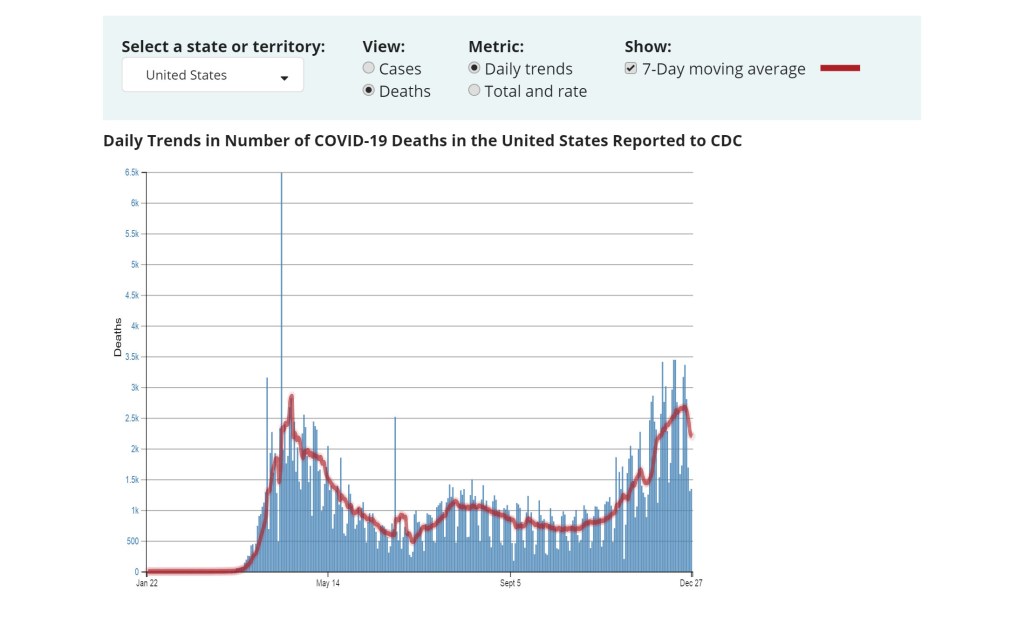
Figure 6: The number of daily deaths in the U.S. from the COVID pandemic vs. time. Near the end of December, nearly 3,000 people per day are dying from COVID; this is roughly the number that died in the 9/11 terrorist attacks on the World Trade Center.

Figure 7: The total number of deaths in the U.S. from the COVID pandemic vs. time (left scale), and the death rate per 100,000 people from the pandemic (right scale). From the CDC.
Figure 8 plots death rates per million inhabitants for various countries. It is useful to introduce some consideration of the differing age distributions among inhabitants, since the mortality rate of the virus increases so rapidly among the elderly. Thus, in addition to plotting the total number of confirmed COVID deaths divided by the total population of each country in Fig. 8 (orange bars), we have also divided (blue bars) by the population aged 70 and above, based on the percentage of elderly inhabitants indicated by 2015 global demographics. For example, Brazil has nearly the same overall death rate as the U.S., but Brazil’s population skews significantly younger, so its death rate among the elderly is quite a bit higher. The U.S. has the second highest death rate among the elderly, among the 15 industrialized nations included in Fig. 8. Note the logarithmic horizontal scale in Fig. 8, where each vertical line represents a factor of 10 change in the death rate. Thus, the elderly death rate per capita in the U.S. is a factor of 100 higher than that in New Zealand or Japan, and a factor of nearly 10 higher than that in Germany.
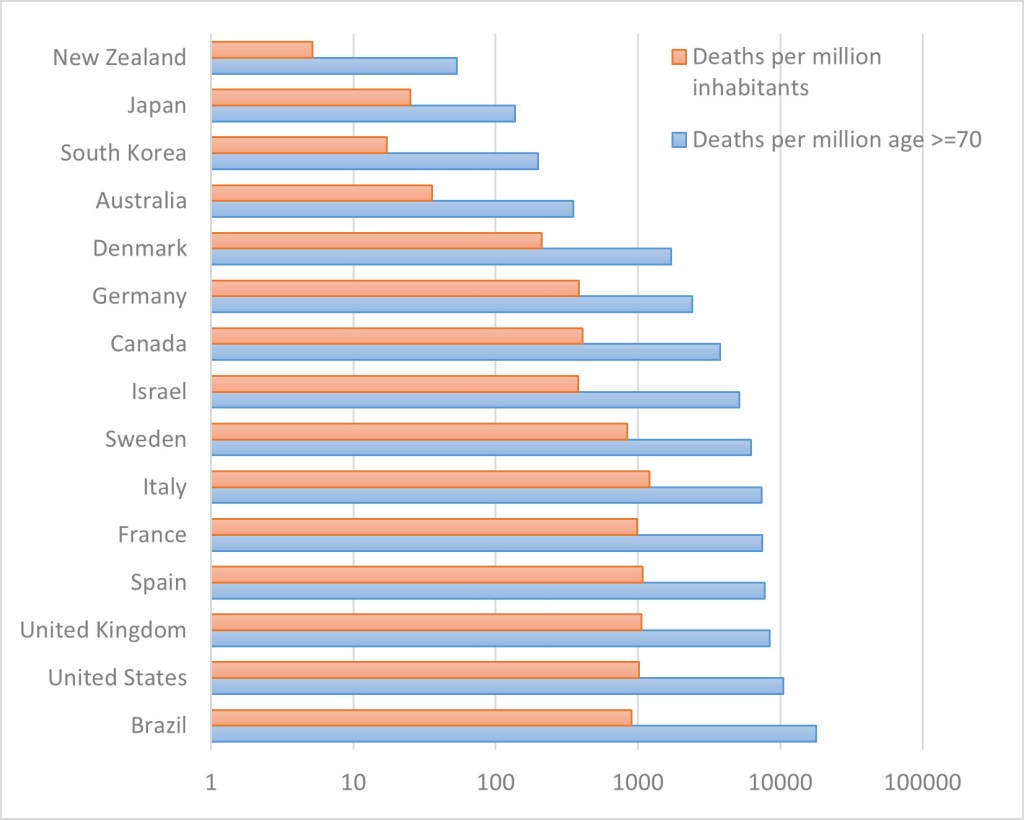
Figure 8: Death rates from COVID-19 per million people, for several countries. Note that the death rates are plotted on a logarithmic scale, where every scale marker represents a factor of 10 difference in the death rates. Orange bars: overall death rates; blue bars: deaths relative to the over-70 part of the population.
Another tactic of the deniers was to claim that the medical community was mis-diagnosing minor ailments as COVID-19, in order to increase payments to doctors and hospitals. Similar claims were made that the number of COVID deaths was grossly over-estimated, because the medical community wanted to use the pandemic as an excuse to take civil liberties away from citizens. It was also claimed a cure for the SARS-CoV-2 virus already existed, but that doctors refused to offer it. It was falsely asserted that hydroxychloroquine was an effective cure for the disease, but that doctors refused to prescribe it because it was too inexpensive. Several of our earlier blog posts (here, here and here) have reviewed the situation with the anti-malarial drug hydroxychloroquine. After a number of physicians suggested that the drug was effective with COVID patients, it became a cause celebre with Fox News commentators and subsequently with Donald Trump. Based largely on their hyping of this drug, the Food and Drug Administration gave it emergency-use authorization. However, subsequent large-scale blinded trials showed that the drug provided little if any relief against COVID; thus the FDA rescinded the emergency-use authorization. However, both the Fox News talking heads and Donald Trump continued to hype this product, long after its merits were debunked by scientific studies.
So the Libertarian community as a whole downplayed the severity of COVID-19, since acknowledgment of the true effects of the pandemic would require that they support global efforts to combat the disease, and might also require that they support temporary restrictions such as mask-wearing, social distancing, and closure of establishments associated with “super-spreader” events, to prevent spread of the disease from overwhelming hospitals and first-line medical responders.
This COVID-denialism has been particularly striking from Fellows of the Hoover Institution for War, Revolution and Peace. This organization was initially established in 1919 when Herbert Hoover donated $50,000 to Stanford University in order to assemble a collection of documents and books dealing with World War I. Funded primarily by private gifts, the Institution eventually built a massive tower on the Stanford campus that housed the library and staff of the Institution.
Figure 9: The central tower of the Hoover Institution on the Stanford University campus.
Although at one time it was autonomous to Stanford University, in recent years the Hoover Institution has developed a close connection to Stanford. Fellows of the Hoover Institution are generally provided with Stanford faculty appointments. During the Trump Administration, a number of Hoover Institution Fellows have either been given appointments in the administration, or have served as consultants to various federal offices. As might be expected from an organization that champions free-market solutions to political and economic issues, the Hoover Institution Fellows have been quite vocal in espousing Libertarian responses to the pandemic. They have also made a number of notable predictions about the coronavirus. We will discuss three of these senior Hoover Institution Fellows and review their coronavirus predictions.
Richard Epstein and the Pandemic:
Richard Epstein is a professor at the New York University School of Law, where he is the Laurence Tisch Professor and director of NYU’s Classical Liberal Institute. Epstein was profiled in our blog post on Science Denial and the Coronavirus. He is also the Peter and Kirsten Bedford Senior Fellow at the Hoover Institution. On March 16 2020, Epstein published a Hoover Institution paper called Coronavirus Perspective. In that paper, Epstein criticized the World Health Organization for calling the disease a pandemic. He famously predicted that the total U.S. death toll from COVID-19 would not exceed 500 people (the death toll on Mar. 16 was only a handful of people).
Figure 10: Richard Epstein, the Peter and Kirsten Bedford Senior Fellow at the Hoover Institution.
A few days later, when the U.S. death toll had already exceeded 500, Epstein claimed that the number 500 was “a simple mathematical error;” he then revised his prediction to 5,000 total U.S. deaths and 50,000 deaths worldwide. A few weeks later, when that number had been surpassed, Epstein further revised his prediction to 50,000 U.S. deaths. As the death toll climbs, Epstein continues to amend his predictions, which are apparently meaningless as he can “update” them in hindsight to any number he likes – they are no longer “predictions” if they are revised after the fact.
It is worthwhile to note that Epstein’s estimates of deaths are based on his allegation that as a virus disease moves through a population, the virus mutates to less and less lethal forms. And the more deadly the initial virus, the faster it will mutate to less virulent forms. Epstein insists that this model for the spread of a viral disease fits every pandemic that preceded the coronavirus. However, Isaac Chotiner, a reporter for the New Yorker, interviewed a number of epidemiologists, all of whom said that Epstein’s theory regarding epidemics was completely wrong. In particular, they stated that this claim was false for both HIV and Ebola. However, Epstein has no hesitation in advocating responses to the pandemic that are based on debunked “medical” theories. Furthermore, he has consistently opposed centralized responses to the pandemic. Epstein claimed that public health measures against the disease “are done better at the level of plants, hotels, restaurants and schools than remotely by political leaders.” Apparently Epstein’s contrarian views were highly valued because they gibed with the political biases of the Trump Administration.
Michael Levitt, Coronavirus Gadfly:
One of the most quotable Hoover Institution Fellows is Stanford biology professor Michael Levitt. Levitt is a world-renowned scientist who shared the Nobel Prize for Chemistry in 2013, for “the development of multiscale models for complex chemical systems.” Levitt arrived at Stanford in 1987 and has since split his time between that university and the Weizmann Institute of Science in Rehovot, Israel.

Figure 11: Prof. Michael Levitt, a biologist who shared the 2013 Nobel Prize for Chemistry. Levitt is a Fellow of the Hoover Institution.
Dr. Levitt is an absolute fountain of predictions regarding the coronavirus. On Feb. 7, 2020, Levitt predicted that “by Feb 14, we will have reached 95% of the eventual death toll of 928 in China” (note that Levitt is willing to predict the exact death toll, a practice that should activate the ‘bullshit detector’ of the reader – see our earlier blog post on this topic). As of Dec. 15, the reported Chinese death toll is over 4,600, and it is widely believed that the actual number of Chinese COVID deaths is much higher. Beginning in March of 2020, Levitt’s take-away was “COVID-19 is not a threat, and the pandemic is over.” On March 20, Levitt stated that he “will be surprised if the number of deaths in Israel surpasses 10.” Furthermore, Levitt used his stature as a Nobel Laureate to speak directly with Prime Minister Netanyahu to convey his message that Israel was over-reacting to the coronavirus. As of Dec. 3, there have been 2,883 deaths in that country. Levitt then said that his earlier estimate was a simple mistake. On March 28, Levitt announced that the pandemic in Italy had passed its peak and would end with no more than 20,000 deaths; Italy now has over 58,000 COVID-19 deaths.
Levitt has suggested that the number of COVID deaths is greatly exaggerated. He claims that it should be possible, and even desirable, for the population to achieve herd immunity naturally, without a vaccine, by letting the disease sweep through the population. He has even proposed that people might infect themselves and thus achieve immunity from the disease by going on a COVID cruise!
Epidemiologists have requested that Levitt provide them with the computer program that he uses to estimate COVID fatalities, so that they can run it to reproduce his predictions. To the best of our knowledge, he has not produced the code. This is no surprise, as his “predictions” have been wildly below the actual cases and deaths from COVID. Sadly, he is using the fame from his Nobel Prize and his stature as a Hoover Institution Fellow to make predictions that are apparently being taken seriously by governments trying to deal with the pandemic. As might be expected, Levitt’s views on the pandemic are widely quoted by Libertarians and COVID deniers.
Scott Atlas and the Great Barrington Declaration:
As we mentioned earlier, the Great Barrington Declaration received a great deal of attention in the national press. Part of this was due to the fact that Dr. Scott Atlas, a senior fellow of the Hoover Institute on War, Revolution and Peace at Stanford University, widely publicized this document. Scott Atlas is a neuroradiologist, who was Chief of Neuroradiology at the Stanford School of Medicine from 1998 to 2012. Dr. Atlas has been a senior advisor for health care for Republican candidates for President, including Rudy Giuliani in 2008 and Mitt Romney in 2012. Dr. Atlas is the author of four books on health care policy. He is an opponent of the Affordable Care Act, he has called for “aggressive reforms” to Medicaid with the aim of turning that program into “a bridge for private insurance,” and he is a strong proponent of medical savings plans.
Figure 12: Dr. Scott Atlas, a neuroradiologist and Senior Fellow of the Hoover Institution.
At the time that the Great Barrington Declaration was written, Scott Atlas was a White House advisor on the Coronavirus. Atlas invited the authors of the Great Barrington Declaration to meet with President Trump. The authors of the Great Barrington Declaration had much in common with Atlas’ stated views on the pandemic. Dr. Atlas had stated in an interview, “We can allow a lot of people to get infected. Those who are not at risk to die or have a serious hospital-requiring illness, we should be fine with letting them get infected, generating immunity on their own, and the more immunity in the community, the better we can eradicate the threat of the virus.”
Dr. Atlas had also strongly pushed other responses to the coronavirus pandemic. He had proposed that non-symptomatic people not be tested for COVID. In August 2020, this position was recommended by the CDC. It was opposed by many in the epidemiological community, particularly because a very large number of people with COVID are asymptomatic, and hence can transmit the disease without ever knowing that they are infected. Atlas was also a major skeptic regarding the idea that wearing masks prevents transmission of the disease. One of his Twitter posts in October 2020 was removed because he falsely claimed that masks do not prevent the spread of the coronavirus (his Tweet began: “Masks work? NO.”). Atlas was also a foe of economic lockdowns in an effort to control the spread of the disease. He revealed his true motives (i.e., that he was acting more out of political leanings than purely medical ones) when he urged residents of Michigan to “resist” or to “rise up” against restrictions designed to slow the spread of COVID-19.
On Thursday, November 19, the Stanford Faculty Senate condemned Dr. Atlas’ actions regarding the coronavirus. A resolution was introduced that criticized Atlas for “promoting a view of COVID-19 that contradicts medical science.” The resolution cited the following actions by Atlas: “disparaging the use of masks and other protective measures, misrepresenting knowledge and opinion regarding the management of pandemics; endangering citizens and public officials; showing disdain for established medical knowledge; and damaging Stanford’s reputation and academic standing.” The resolution concluded that Dr. Atlas’ behavior was “anathema to our community, our values and our belief that we should use knowledge for good,” and it was approved by 85% of the Faculty Senate.
Stanford’s president Marc Tessier-Lavigne stated that he was “deeply troubled” by Dr. Atlas’ remarks, and he said that “We’re therefore compelled” to distance Stanford from Dr. Atlas’ views. Condoleezza Rice, the current Director of the Hoover Institution, also said that Dr. Atlas’ tweet calling for citizens to “rise up” against public-health restrictions in Michigan was “offensive and well beyond the boundaries of what is appropriate for someone in a position of authority.”
It is clear that the public remarks by Dr. Scott Atlas are motivated more by his political beliefs than by solid science about the coronavirus. Although Atlas is a renowned radiologist, he has no expertise in epidemiology. Furthermore, his claim that we should encourage young people and those without compromised immune systems to be infected with the disease is a position that is strongly opposed by the great majority of the public-health community. The measures supported by Dr. Atlas would needlessly expose many people to death or serious injury from the SARS-CoV-2 virus. His proposed actions violate the dictum for physicians “first, do no harm” that has been attributed to Hippocrates. Furthermore, achieving the goal of herd immunity in the absence of a vaccine would likely lead to more than 1 million American deaths before this goal could be achieved. It is no wonder that Dr. Anthony Fauci and Dr. Deborah Birx of the Coronavirus Task Force were strongly opposed to Atlas’ comments. In fact, Birx apparently complained to Vice President Mike Pence about the misinformation provided by Dr. Atlas, and recommended that he be removed from the Coronavirus Task Force.
Libertarians argue that the economy should continue much as it had before the pandemic. They further denigrate public-health measures to slow the spread of the disease; Richard Epstein argued that public-health decisions are best done “at the level of plants, hotels, restaurants and schools,” rather than by governments. And all three Hoover Institution Fellows advocate letting the virus “sweep through the population,” claiming that this will rapidly lead to herd immunity. Several countries have been extremely successful in stopping the spread of COVID, and re-opening their economy. All of these share two common features: first, their response was coordinated by a strong central government; and second, they followed the advice of scientists in determining when to shut down the economy and when to re-open. These are also the conclusions reached by the many simulations of epidemics. The Libertarian arguments completely contradict these lessons. We should remember that no pandemic has ever been solved by using herd immunity as a goal, in the absence of a vaccine.
How Well Has the U.S. Managed the Coronavirus Pandemic?
We covered this topic in earlier blog posts on science and the coronavirus that can be found here, here and here.
For the past 20 years, groups of scientists and government officials have run simulations of natural disasters. The purpose is to discover what steps need to be taken when a disaster arises. Since previous administrations realized the high probability of a future epidemic, they underwent extensive planning for such a public health emergency. They ran simulated exercises for hypothetical outbreaks, to test their preparedness for such catastrophes. They collected the results of these simulations in “playbooks” that listed the steps required to contain such an outbreak, tabulated those actions that were successful and highlighted the potentially weak links in supply chains and public-health infrastructure. A major simulation of a global pandemic took place in New York City in October 2019, under the leadership of Ryan Morhard of the World Economic Forum.
There were two major takeaways from simulations of epidemics. First, it was essential that steps to mitigate the spread of the disease be taken at the very first sign of a possible pandemic. Delays of even a few days could allow the disease to spread like wildfire through the population. A second lesson from the simulations was the necessity to coordinate action to account for every link in logistical supply chains. Shortages of even seemingly trivial elements of protective gear or medical supplies could seriously impact the response to an epidemic.
When the Trump Administration was first apprised of a new infectious disease that apparently originated in Wuhan, China, they fairly rapidly initiated a ban on flights from China to the U.S. The ban was announced on Feb. 2, 2020. However, that ban was “leaky” in that some 40,000 people flew from Wuhan to the U.S. over the next few months. But the flight ban nevertheless provided some positive benefits in responding to COVID-19.
However, over the next several weeks, the U.S. failed to take decisive action to stop the spread of the coronavirus. A major part of that inaction was Donald Trump’s desire to take personal credit for preventing the pandemic from spreading through the population, and his insistence on being seen as ‘in control’ of the situation. Throughout January and February, Trump insisted that the U.S. would not experience any serious health problems from the coronavirus. On Jan. 22, he stated, “We have it totally under control. It’s one person coming in from China, and we have it under control. It’s … going to be just fine.” And on Feb 2, Trump told Fox News host Sean Hannity, “We pretty much shut it down coming in from China.” On Feb. 14, Trump told a group of Border Patrol agents: “We have a very small number of people in the country, right now, with it. It’s like around 12. Many of them are getting better. Some are fully recovered already. So we’re in very good shape.”
On Feb. 25 Nancy Messonnier, the Director of the National Center for Immunization and Respiratory Diseases at the U.S. Centers for Disease Control, warned in a White House briefing of the impending community spread of the virus within the U.S., predicting that “Disruption to everyday life might be severe.” In response, Trump tweeted that the virus “is very much under control.” Then on Feb. 27, Trump claimed that the virus would be temporary. “It’s going to disappear. One day, it’s like a miracle – it will disappear!” He continued on this theme for the next nine months, even as the coronavirus swept across the U.S. A significant issue was the Trump Administration tendency to see the pandemic more as part of Trump’s re-election strategy (Trump is in charge; we have it under control; don’t panic; go about your business as usual) than as a public-health emergency. Look at Figs. 5-8 to see if COVID-19 has “disappeared” in the U.S. by the end of 2020.
Even after the administration finally acknowledged the seriousness of the epidemic in mid-March and began holding daily briefings of the Coronavirus Task Force, Trump systematically undercut the recommendations of his own scientists, downplayed the seriousness of the virus, and sowed confusion about the best ways to protect against SARS-CoV-2. By March, epidemiologists were virtually unanimous that wearing masks in public and exercising social distancing were essential to “flattening the curve.” However, Trump announced that he would not personally wear a mask. In numerous public appearances during March through May, Trump was never seen wearing a mask, and he rarely enforced social distancing in public. In fact, an event to introduce Supreme Court nominee Amy Coney Barrett in the White House Rose Garden became a “super-spreader” event that caused at least a dozen people to become infected with COVID, including President Trump himself.
Because of the confusion sowed by the President and his supporters, bad planning by the federal government and poor coordination with state agencies, and the politicization of measures to slow the spread of the disease, the U.S. has one of the highest per-capita death rates in the world. In a review of the U.S. pandemic response in the journal Nature, Amy Maxmen and Jeff Tollefson question “Why did dozens of simulations, evaluations and white papers fail to predict or defend against the colossal missteps taken in the world’s wealthiest nation?” Their answer is presaged in the abstract to their article: “Two decades of war-game scenarios foresaw leaky travel bans, a scramble for vaccines and disputes between state and federal leaders. But none predicted Donald Trump.”
However, many Trump supporters claim that Donald Trump’s actions saved millions of people from dying. How can we quantify the results of the U.S. government’s response to the coronavirus pandemic? As we mentioned earlier, if no actions were taken to slow or halt the spread of the virus through the American population and no vaccine was available, the disease would likely kill more than 1 million Americans before herd immunity was achieved. On the other hand, we can estimate the number of Americans that would have died from COVID if this country had mounted an effective defense against the pandemic.
Consider those countries that mounted an effective defense against the coronavirus. These are countries such as South Korea, Vietnam, Taiwan, Australia, Singapore and New Zealand. We can take the number of deaths in those countries, scale up those deaths to an equivalent population of the U.S., and thus obtain the number of deaths if those countries had the same population as we do.
For example, on June 19, Isaac Sebenius and James K. Sebenius address the following question: Had American leaders taken the decisive, early measures that several other nations took when they had exactly the same information the U.S. did, at exactly the same time in their experience of the novel coronavirus, how many of these Covid-19 deaths could have been prevented?
The Sebeniuses carried out the following calculations. They compared the U.S. response with that of South Korea, Australia, Germany and Singapore. They scaled the population sizes and COVID-19 deaths to match those of the U.S. And they noted that the pandemic occurred earlier in those countries than the U.S., which gave our government more information to guide decision-making. They applied a “stringency index” developed at Oxford University to measure the speed at which the countries responded, using 14 days from the 15th confirmed COVID case as a comparison date.
The results were as follows. In the four months following the 15th confirmed case, and scaling up each country to produce equal populations, a US-sized Germany would have had 35,049 COVID deaths, compared with 1,758 equivalent deaths in South Korea, 1,324 deaths in Australia, and 1,358 deaths in Singapore. Compared with the 117,858 U.S. deaths in those four months, Sebenius and Sebenius conclude that between 70% and 99% of those American deaths could have been prevented, had the U.S. acted as rapidly as those countries. Results of these simulations should be taken with some caution because of uncertainties in the model. However, the results suggest that between 82,000 and 116,000 of the American COVID deaths through mid-June occurred because of the failure of the Trump Administration to act rapidly and comprehensively, when they first became aware of the epidemic.
The estimates in this article are in line with other attempts to estimate the number of unnecessary American deaths due to the coronavirus, using different methodologies. An epidemiological model by a Columbia University group simulating the spread of the disease estimated that if the U.S. response had begun two weeks earlier than it did, 80% of the fatalities could have been avoided. And a similar epidemiological model for disease transmission used by Britta Jewell and Nicholas Jewell estimated that up to 90% of the deaths could have been avoided, if lockdowns and social distancing had begun two weeks earlier.
So the truth is that many experts and non-experts did indeed foresee just such a global pandemic. One journalist even presciently predicted, before the 2017 inauguration, that Trump’s response to such a pandemic would be highly problematic and feature extensive misinformation. Writing in The Atlantic in December 2016, Ed Yong speculated: “As Donald Trump prepares to become America’s 45th President in January 2017, the question isn’t whether he’ll face a deadly outbreak during his presidency, but when? And more importantly, how will he cope?… If anything, this problem is likely to get worse, given America’s continuing struggle to deal with ‘fake news.’ Inaccurate information can be easily seeded by foreign parties, and given weight and prominence by online algorithms. It’s arguable whether such misinformation made a difference between victory or defeat in the election, but inarguable that it could mean life or death in an outbreak.”
The U.S. has 4.3% of the world’s population, but nearly 25% of its confirmed COVID-19 cases. Its per capita COVID death rate is among the highest in the world, as illustrated in Fig. 13. This figure gives the COVID death rates per million people for various countries through Dec. 31, 2020. Note that the U.S. rate is about 100 times larger than countries such as Australia, Japan and South Korea.
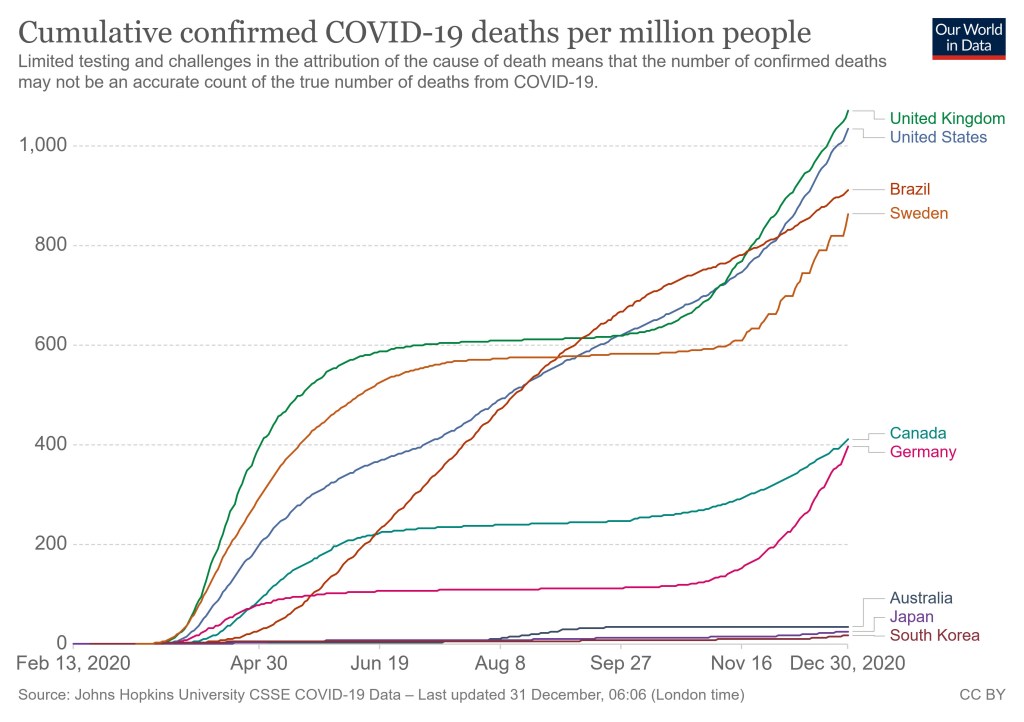
Figure 13: Cumulative deaths from COVID per million people for various countries, through Dec. 31, 2020.
Estimating the number of unnecessary American COVID deaths is not an exact science. From the estimates that we have given, that number could vary anywhere from 40,000 to 250,000 deaths that could have been avoided, had the U.S. taken the same steps as relatively successful countries such as South Korea, Australia, New Zealand, Vietnam and Taiwan. The number of COVID-19 deaths in the U.S. is nearly 340,000 as of Dec. 29, 2020; as we have mentioned, no other country in the world has as many deaths as the U.S., and we also have one of the highest per capita death rates in the world. Apportioning the blame for this scandalously high number of deaths is still more difficult. However, it seems inescapable that the Trump Administration, and Donald Trump personally, are to blame for many of these deaths. For several weeks at the beginning of 2020 the Trump Administration refused to act swiftly, instead relying on Trump’s assertions to Fox News commentators that the disease was “completely under control.” When the Coronavirus Task Force began operations, Trump refused to invoke the Defense Production Act for the purpose of manufacturing and delivering all the person protective equipment needed by first-line providers. After the Coronavirus Task Force issued a set of guidelines for slowing the spread of the disease (including wearing masks and social distancing), Trump himself refused to wear a mask, and hosted several events where social distancing was not practiced. Trump also urged governors to re-open their states before they had satisfied the criteria specified by the CDC.
And finally, during the summer of 2020 Trump decided that the best strategy for his re-election campaign would be to ignore the pandemic altogether. He minimized the spread of the disease across the country, and repeatedly insisted that COVID-19 was “going to disappear.” He hardly mentioned the pandemic during his political rallies, and he brought it up at his increasingly infrequent press conferences only when he was asked pointed questions by reporters. Trump also tweeted misinformation about the pandemic from right-wing commentators, quack medical personnel (remember ‘America’s Frontline Doctors’?), and continued to tout the anti-malaria drug hydroxychloroquine, even after the largest medical trials showed that the drug had no positive effect on treating COVID patients, and the FDA had revoked its emergency-use authorization for treating COVID. At one point, he even raised the idea that ingesting bleach or shining ultraviolet light inside the body might be effective ways to kill the virus.
At the same time, political appointees were scrutinizing material on the pandemic released by Health and Human Services and the Centers for Disease Controls, and attempting to suppress or modify data or public statements that they deemed were in conflict with any claims made by the White House. Thomas Caputo, the former top communications official at the Dept. of Health and Human Services, claimed that government scientists were “engaging in ’sedition’ in their handling of the pandemic.” Caputo also accused the CDC of containing a “resistance unit” that was deliberately working to undermine President Trump. The heavy-handed political interference into their efforts has seriously damaged the reputation of both the Centers for Disease Control and the Food and Drug Administration. It has definitely contributed to the wariness of the American public to trust public statements from those departments.
Now that we have at least two vaccines against the SARS-CoV-2 virus, it looks as though the U.S. can finally look forward to putting the pandemic behind us. In particular, Pfizer and Moderna have successfully produced vaccines that employ the new messenger RNA technique. At the moment, the development, testing and production of these new vaccines appears to be an extremely good example of a partnership between basic research groups, private pharmaceutical companies, and the federal government. The Trump administration provided many financial incentives to these efforts (though not to the Pfizer developments) through Operation Warp Speed, and the new vaccines were produced at record speed.
The eventual success of the vaccines against COVID-19 will now depend on several factors. First, it is hoped that the vaccine will be successful at the 90% rate or better, as was shown in clinical trials. Second, the vaccines need to be administered to the public as fast as possible; apparently Operation Warp Speed was only concerned with manufacturing the vaccine and is leaving administration to individual states, while the Trump administration claims they have absolutely no role to play in planning and coordinating a nationally efficient vaccination program. Third, the vaccines will be widely accepted only if there are no quality-control issues in manufacturing and distributing the vaccine. Public acceptance will also depend on having only a small number of adverse reactions from the vaccine. In the first few days, there have been a couple of reports of people who experienced a strong allergic reaction to the vaccine. However, such reactions are easily treatable if people notify physicians of their status prior to receiving the vaccine. The allergic reactions appear immediately, within a few minutes of the injection.
One potentially serious issue is whether enough people will get the vaccine so that the U.S. can acquire ‘herd immunity’ against COVID. Earlier, we gave a rough estimate that at least 60% of the population needs to have immunity (either by having had the disease or being vaccinated), so that the epidemic is unable to spread through the population. There are two factors mitigating against getting people vaccinated. One is that the disastrous U.S. response to the coronavirus has made Americans increasingly wary of health-related statements by the government. A recent study showed that 39% of Americans said that they would ‘definitely’ or ‘probably not’ take the vaccine. However, half of that group said that they might change their minds once more information was available. And that number was down from the 49% who said they would not take the vaccine in earlier polls.
However, there are large and growing anti-vaccination groups that are launching major disinformation campaigns on social media, to undermine public confidence in the coronavirus vaccines. First, the disastrous U.S. response to the COVID-19 pandemic has left many people suspicious of any programs backed by the government. Anti-vaxxers have been very successful in creating online Web sites that spread false information about the pandemic, and about vaccines. What was once primarily an American anti-vaxxer community has recently become a worldwide phenomenon.
Anti-vaccination efforts take several different forms. The first is the claim that the pandemic is not serious, and that the ‘natural’ form of immunity gained through getting the disease is ‘better’ than vaccination (we will deal with this claim in the next section). A second attack claims that the vaccines will be ineffective against the disease, regardless of the evidence from clinical trials. And a third claim is that the vaccines are actually dangerous; that they will cause more harm than good. The claim that vaccines do more harm than good is powerful because it is connected to conspiracy theories that spread disinformation or mistrust in government and powerful elites. So, for example, many anti-vaxxer sites claim that the vaccine is being promoted by people like Bill Gates to make more profits, or to realize his dream of implanting microchips in people to track their movements. Anti-Semitic sites claim that the vaccines (or even the pandemic itself) are a plot by wealthy Jews – for example, many anti-vaxxer sites are now claiming that George Soros is behind efforts to push vaccines.
Other groups claim that Big Pharma and wealthy doctors are hyping vaccines in order to make more profits. It also appears that QAnon groups are expanding their activity to include anti-vaccination arguments, and vice versa. For example, Larry Cook and his private Facebook Stop Mandatory Vaccination site were recently removed from Facebook for promoting the QAnon conspiracy theory (which was covered in a previous post on our blog site). The anti-vaxxers see the controversy regarding the COVID-19 pandemic as a way not only of connecting with people concerned about taking the new vaccines, but of expanding those efforts to convince people to resist all vaccines, especially childhood vaccinations.
One of the leading anti-vaccination spokespersons is Robert Kennedy Jr. Kennedy is Chairman of a group called Children’s Health Defense. That group has lobbied against childhood vaccination, fluoridation of drinking water, and acetaminophen, among other things. We reviewed Kennedy in our blog post on vaccination. Although he claims that every statement he makes is carefully fact-checked, a piece Kennedy wrote for Salon called Deadly Immunity was retracted after Salon encountered numerous false statements. Lately, Kennedy has become an international spokesperson for the anti-vaxxer movement. He now appears willing to spread baseless rumors about not only vaccines, but whether Bill Gates is attempting to insert microchips into individuals so they can be tracked by the state. He has also claimed that Dr. Paul Offit, one of the leading virologists in the world, was an “enabler” of a vaccine-autism “Holocaust,” and he stated that Offit and fellow virologists “Should be in jail and the key thrown away.”
Figure 14: Robert F. Kennedy, Jr., one of the leading anti-vaccination activists.
If the anti-vaxxers succeed, a large number of people will decline to get the vaccine. This could prevent the U.S. population from achieving herd immunity. If this were the case, then the coronavirus could become endemic in the U.S. If too few people acquire immunity through vaccination, then the coronavirus would cycle through the population at regular intervals. Society will have to deal with the tricky issue of countering the lies and misinformation that will cycle through social media. It remains to be seen if a balance can be struck between freedom of speech, and protection of the populace from the harm that is done by the dissemination of false information. As we have experienced in the four years of the Trump Administration, there is no simple answer for how to deal with false information on social media. We will see whether the scientific community, or the anti-vaxxers, manage to prevail on the issue of the COVID vaccines.
Is Infection ‘Better’ than Vaccination in Providing Immunity Against COVID?
In this section we will consider a claim made by anti-vaccination groups, that has also been raised by people who claim that the risks from the coronavirus are exaggerated. This is the statement that immunity conferred by vaccination is somehow “weaker” or “shorter-acting” than the immunity one acquires after being infected by a disease. For example, after two pharmaceutical companies announced their findings from tests of their vaccines, U.S. Senator Rand Paul tweeted that the Pfizer and Moderna groups had announced that their vaccines were 90% and 94.5% effective against the SARS-CoV-2 virus. But, noted Sen. Paul, “naturally acquired” COVID was 99.9982% effective. Senator Paul, who himself had contracted COVID, “has argued that surviving a bout of Covid-19 confers greater protection, and poses fewer risks, than getting vaccinated.” His efficacy claim has no basis in research on COVID-19, and apparently the 340,000 American deaths to date, and the possibilities of long-term health problems, from the disease represent a minimal risk in Paul’s Libertarian estimation.
To answer this question we need to consider the risks and rewards associated with vaccination vis-a-vis those from acquiring the disease. In the case of COVID-19, the answer is clear. Dr. Jennifer Gommerman, an immunologist from the University of Toronto concludes that choosing this disease over getting vaccinated would be “a very bad decision.” A carefully-chosen vaccine will be both safe and predictable. It will provide every patient with the same dose of vaccine; this is designed to produce a substantial immune response. Furthermore, the vaccines have been tested in tens of thousands of people before being authorized for use by the public. Severe adverse reactions from the vaccine are expected to be in the range of 1 for every 100,000 to one million people, and deaths directly attributed to vaccination are generally in the range of 1 for every 10 million vaccinations.
On the other hand, getting COVID-19 involves much greater risk. University of Florida biostatistician Natalie Dean pointed out, “The key distinction is that vaccines are a SAFE way to achieve immunity. Getting sick with COVID-19 is inherently unsafe. We would never tolerate a vaccine that carried even a fraction of the risks of natural infection.” In a study of over 3,000 people in the age range 18-34 who were hospitalized, 20% required intensive care and 3 died. Furthermore, as many as one person in three who survived a bout of COVID reported chronic issues for months afterwards. Some people have reported long-term issues from COVID that were similar to autoimmune disorders such as lupus and rheumatoid arthritis. And even people whose COVID symptoms are very light are capable of passing the disease along to friends and relatives who may be much more at risk from the disease. Comparing infection by COVID with vaccination, immunologist Marion Pepper of the University of Washington states “It’s clear that … there’s more risk with natural infection.”
People who contract COVID also receive viral loads that vary greatly. People who are asymptomatic or who have very mild symptoms may produce few or no antibodies. In those cases, the individuals may be at risk for being re-infected with the virus. On the other hand, those who receive the vaccine will uniformly produce many virus-fighting antibodies.
Anti-vaccination groups are particularly prone to making these arguments (getting the disease is preferable to vaccination) with respect to measles. They tend to portray measles as little more than a nuisance, with very few adverse effects. In fact, in about 0.1% of measles cases a person will suffer a bad reaction. Even in Europe, with generally advanced medical standards, death occurs in about 0.02% of measles cases; this is a rate thousands of times greater than fatality rates arising from vaccinations.
The Swedish “Experiment” Dealing With the Coronavirus:
Unlike nearly all their counterparts in the European community, and in particular unlike their Scandinavian neighbors Norway, Denmark and Finland, Sweden took a rather unique approach to the coronavirus pandemic. While countries like Norway and Denmark quickly locked down their economies in early 2020, when COVID-19 began to sweep through the population, Sweden chose instead to adopt a much more laissez-faire approach. They let schools and most businesses, restaurants, bars, gyms and other establishments remain open. Although they issued guidelines for personal behavior regarding the pandemic, those guidelines were nearly all voluntary. The one mandatory public-health measure was a ban on gatherings of more than 50 people. Figure 15 below shows people on a beach in Malmo in the summer of 2020. There are hardly any masks and no social distancing to be observed.

Figure 15: Swedish people at the beach in Malmo in summer 2020. Very few masks are in evidence and no social distancing seems to be observed.
The Swedish experiment had two main objectives. The first was a goal of allowing the virus to sweep through the population. Sweden’s top epidemiologist and head of the country’s Public Health Agency, Anders Tegnell, argued that they could achieve herd immunity by allowing many Swedes to contract the disease and hence achieve immunity. The second objective was to prevent their economy from tanking. The Swedes thus expected that their economy would suffer a substantially smaller contraction than their neighbors, e.g., Norway and Denmark.
For a short period in early spring of 2020, it appeared that the Swedish experiment might have some benefits. The earliest data suggested that the Swedish economy might be impacted less than that of their neighbors. However, the COVID death rate in Sweden was extremely high. Their per-capita death rate was nearly ten times greater than that of Norway, 7 times greater than Finland and 6 times more than Denmark. The Swedish per-capita death rate was even 40% greater than that in the U.S., which has one of the larger per-capita COVID-19 death rates in the world.
Nevertheless, many conservatives in the U.S. looked to the Swedish experience as an example of the correct response to the pandemic. Since they seem to value economic prosperity and individual liberties more than the lives of the citizens involved, they extolled the Swedish experiment. They anticipated that over the next several months, Sweden’s economy would remain relatively vibrant while most world economies had gone into deep recession. Many conservatives watched Sweden intently, to see how their economy fared.
Many of the conservatives who championed herd immunity also lauded Sweden for their refusal to lock down the economy, and their reliance on purely voluntary restrictions on behavior and public assembly. As for the shockingly high COVID death rates in Sweden? “Watch and learn,” they said. “In late fall, the second wave of COVID will hit Europe. At that time, the Swedes will have come much closer to achieving herd immunity than their neighbors. While the rest of Europe experiences steep increases in second-wave infections, there will be far fewer COVID cases in Sweden.”
We now have firm data on what happens to a country that allows society to carry on much as usual in the face of a virus like SARS-CoV-2. As to the economy, researchers have compared the economic impact in Denmark and Sweden from mid-March to early April. This was the period where the Danes locked down their economy. They found that spending in Denmark during this period had contracted 29 percent, while Sweden’s decrease in spending was 25%, nearly equal to that in Denmark. This illustrated that the contraction in the economy was dictated more by the coronavirus than by government economic policy. Despite Sweden’s leaving their businesses open, many people voluntarily decreased their spending, while decreases in global trade impacted Sweden as much as its neighbors. In addition, global supply chains shut down, which also impacted Sweden greatly.
So the expected economic advantage helped Sweden for a few weeks in early 2020, but afterwards their economy fared about as poorly as their Scandinavian neighbors. Economic forecasts have the Swedish economy contracting by about 4.5 percent this year; this can be compared with an expected contraction of 4.1 percent in Denmark. This is shown in Fig. 16, which compares effects on gross domestic product (GDP) for the second quarter of 2020, vs. deaths per million population for the four Scandinavian countries. As can be seen, the change in GDP is very similar for all four countries.
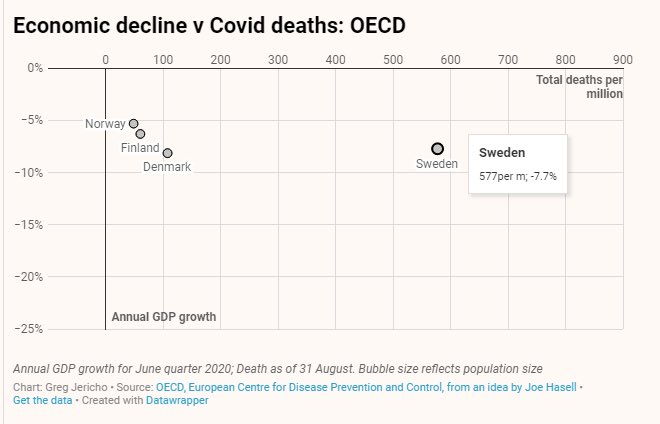
Figure 16: Change in GDP (vertical axis) for June quarter 2020 vs. deaths per million inhabitants for the Scandinavian countries Norway, Denmark, Finland and Sweden. Data through Aug. 31, 2020.
But what about the second wave of the coronavirus? Is it true that Sweden is seeing far fewer COVID cases this fall than their counterparts? Unfortunately, the answer is a clear “No:” Sweden is currently experiencing even more new COVID cases than their neighbors. This can be seen from the very rapid rise in Swedish deaths in the last few months, shown in Fig. 13. In November, positivity rates in testing in Stockholm were at about the 20% level. Hospitalizations in Sweden were rising faster than in any other European country. “So far Sweden’s strategy has proven to be a dramatic failure,” said Swedish virologist Lena Einhorn. “Four days ago we had eight times higher cases per capita than Finland and three and a half times more than Norway.” So much for herd immunity. Figure 16 shows the COVID deaths per million people in the Scandinavian countries. Note that Sweden’s death rate is about six times that of Denmark and nearly 10 times that of Norway.
On Dec. 16, King Gustaf XVI of Sweden told the state broadcaster SVT, “The people of Sweden have suffered tremendously in difficult conditions. I think we have failed. We have a large number who have died, and that is terrible.” At the time, two major regions of Stockholm and Skane have had to postpone non-emergency operations due to the strains placed on Sweden’s health system by the second wave of COVID. In Skane, the positivity rate for COVID-19 tests was over 25%, and public confidence in government authorities had dropped to 34%, the lowest figure ever recorded. Calls for the resignation of Anders Tegnell and/or Health Minister Lena Hallengren over the failed strategy have been increasing rapidly.
Sweden’s COVID-19 experience is also a blow to right-wing Americans who claim that herd immunity is surprisingly easy to achieve. In the first wave of the pandemic, the Swedes tolerated many more COVID cases than other countries, on the grounds that they would be much better off in the second wave of the coronavirus. In fact, they are worse off than other Scandinavian countries. If herd immunity could be achieved after only 10% of the population contracted the disease (as claimed by many conservatives, including the authors of the Great Barrington Declaration), the Swedes should have avoided a second wave of COVID.
In response to these dire statistics, in mid-November Sweden issued new restrictions on restaurants and bars, protective measures for nursing homes, and bans on gatherings of more than 8 people. Alas, the Swedish experiment, hailed by the right wing in the U.S. as likely the best response to the pandemic, has proved to be one of the worst. Jacob Kierkegaard, a senior fellow at the Peterson Institute for International Economics in Washington D.C., stated “They literally gained nothing. It’s a self-inflicted wound, and they have no economic gains.”
Summary:
Over the past few months, we have seen a widespread movement among conservatives and libertarians suggesting a ‘laissez-faire’ attitude towards the COVID-19 pandemic. Advocates for this position suggested that the best response to the epidemic is one that leaves all businesses and schools open, even in the absence of a vaccine. It was claimed that this would provide the optimum benefits for the economy and for business owners. Under this scenario, individuals could make their own choices as to whether they choose to patronize these establishments. They claimed that if the pandemic was allowed to “sweep through” the population for a few months, this would result in achieving herd immunity, or nearly so, so that the populace is spared from further waves of the coronavirus.
The people supporting these recommendations claim that for most people, the coronavirus is simply an inconvenience with few or no lasting effects. They also claim that young people in the K-12 age range tend to get very mild cases of the disease and they do not transmit the disease readily. Some advocates for this approach even suggest that as many children as possible should be encouraged to get the virus, so that they will obtain immunity and move the community more rapidly towards achieving herd immunity. Such groups also tend to spurn the public-health methods suggested by the medical community, such as wearing masks in public, obeying social distancing, frequent washing of hands and not touching one’s face.
These conservatives suggest that the elderly and those with compromised immune systems should be “shielded” from the rest of the population so that they do not contract the disease; however, no details have been provided as to the mechanism for shielding the vulnerable. The people advocating for these actions claim that their proposals will be of great help to minorities and the poor, as they will not have to provide child care for children involved in online education, and businesses will remain open so they will not suffer financially. However, such families often have living situations where several generations live in close proximity; thus, shielding older vulnerable citizens is harder for those groups.
The Trump Administration welcomed and promoted these proposals, because they were similar to the actions taken by the administration. Although the President’s Coronavirus Task Force and the CDC issued sensible guidelines to slow the spread of the disease, White House officials generally ignored these recommendations. In particular, Donald Trump almost never wore a mask or practiced social distancing, and in fall 2020 he held several large gatherings where very few masks were evident.
In this post, we showed that these proposals are a terrible idea for dealing with the coronavirus. We pointed out that the U.S. response to the pandemic has been disastrous: with only 4.3% of the world’s population, the United States has nearly 25% of the world deaths from COVID-19. We also showed that at least a million Americans would die before herd immunity could be achieved without a vaccine, if in fact immunity is sufficiently long-lasting to even approach herd immunity. That anticipated death toll is twice or more as large as the total number of Americans who died in World Wars I and II combined. Advocates for the ‘natural’ approach claim that herd immunity could likely be achieved after as few as 10% of the population is infected; this is an unjustified and much smaller number than 60% of the population, the number obtained from simple estimates of disease transmission.
We showed that the laissez-faire policies recommended by libertarians would result in many more deaths, and more people suffering long-term health impacts. In particular we emphasized that the Swedish experience with COVID, which was similar in many respects to the response advocated by the right wing, has been a disaster. Relative to their Scandinavian counterparts, the Swedes have experienced nearly identical economic impact from the coronavirus, while the per-capita Swedish death rates have been as much as ten times greater than their neighbors.
The Swedes initially justified their approach by arguing that they might sustain greater deaths during the first wave of the pandemic, but that they would experience a much milder ‘second wave’ than other countries, because they would be much closer to herd immunity. Unfortunately, that prediction turned out to be completely wrong: the Swedes are now experiencing a second wave of infections that is as bad as other countries. One commentator assessed the Swedish response to the pandemic: “They literally gained nothing. It’s a self-inflicted wound, and they have no economic gains.”
Now that we have at least two new vaccines against the coronavirus, the next few months will prove extremely interesting to watch the public acceptance. In an optimistic scenario, the vaccines will prove to be effective. They will protect against the virus with very few side effects. The public will rapidly change their initial skeptical attitudes towards the vaccine, and a very large segment of the population will get vaccinated. By taking the vaccine, the American public will achieve herd immunity, and the epidemic will die out. In the negative scenario, attacks on the vaccine and on the whole concept of vaccination will succeed. Large numbers of Americans will refuse to be vaccinated. As a result, herd immunity will never be achieved and COVID-19 will become endemic in the U.S. The disease will continue to cycle through the population, endangering both the elderly and people who are too young to be vaccinated.
Source Material:
David Jones and Stefan Helmreich, The History of Herd Immunity, The Lancet Sept 19, 2020
Sheldon Dudley, Human Adaptation to the Parasitic Environment, Proc. Roy. Soc. Med. 22, 569 (1929)
Debunking Denial: The Eugenics Movement in the United States
Debunking Denial: Science Denial and the Coronavirus
Debunking Denial: Conservative Alternative Science Confronts, and is Routed By, the Coronavirus
Wikipedia, Great Barrington Declaration
Isaiah Berlin, Four Essays on Liberty, Oxford University Press 1990.
Coronavirus May Have Infected Half of UK Population – Oxford Study. Clive Cookson, Financial Times Mar 24, 2020
COVID-19: Do Many People Have Pre-Existing Immunity? Peter Doshi, BMJ 2020.370.m3563
Britain’s “Professor Re-Open,” Tunku Varajarajan, Wall Street Journal June 5, 2020
New Declaration Calls for ‘Focused Protection’ to Achieve COVID-19 Herd Immunity. Critics Say it Would Be Deadly. Sharon Kirkey, Postmedia News, Oct 8, 2020.
Far More People May Have Been Infected by Coronavirus in One California County, Study Estimates, Michael Nedelman, CNN Apr 20, 2020
How (Not) To Do an Antibody Survey for SARS-CoV-2, Catherine Offord, The Scientist, Apr 28, 2020
Fewer than 1 in 10 Americans Have Antibodies to Coronavirus, Study Finds, Stanford Medicine News Center, Sept 28, 2020
Dr. Fauci Says Letting the Coronavirus Spread to Achieve Herd Immunity is ‘Nonsense’ and ‘Dangerous,’ Noah Higgins-Dunn, CNBC Oct 15, 2020
5 Failings of the Great Barrington Declaration’s Dangerous Plan for COVID-19 Natural Herd Immunity, Stephen L. Archer, The Conversation, Nov 2, 2020
“Herd Immunity” Is Not An Answer to a Pandemic, Infectious Diseases Society of America, Oct 14 2020
Ron Paul, The Coronavirus Hoax. Facebook March 16, 2020.
Fact-Checking Rush Limbaugh’s Misleading Claim That the New Coronavirus is “The Common Cold,” Bill McCarthy, Politifact, Feb 27, 2020.
Don Jr. Dismisses Coronavirus Deaths: ‘The Number is Almost Nothing,’ Quint Forgey, Politico, Oct 30, 2020
Wikipedia, Hoover Institution
Richard Epstein, Coronavirus Perspective, Hoover Institution, Mar. 16, 2020
The Contrarian Coronavirus Theory That Informed The Trump Administration, Isaac Chotiner, The New Yorker Mar 30, 2020
Wikipedia, Michael Levitt
Nobel Laureate: Surprised if Israel Has More than 10 Coronavirus Deaths, Donna Edmunds, Jerusalem Post, Mar 20 2020
Nobel Prize-Winning Scientist Says Coronavirus Outbreaks in New York and Italy are Finally SLOWING, Sa Blanchard, Daily Mail (UK), Mar 30 2020
Lior Pachter, The Lethal Nonsense of Michael Levitt, blog Bits of DNA, Sept 21, 2020
Debunking Denial, How to Tune Your Bullshit Detector
Wikipedia, Scott Atlas
Dr. Scott Atlas, Special Coronavirus Advisor to Trump, Resigns, Vanessa Romo, NPR, Sept. 30, 2020
Masks Work? NO: Twitter Removes Tweet by White House Coronavirus Adviser That Says Face Covering Are Not Effective Against COVID-19, Sophia Ankel, Business Insider Oct 18, 2020
Trump Coronavirus Adviser Scott Atlas Urges Michigan to “Rise Up” Against New COVID-19 Measures, Paul LeBlanc and Jeremy Diamond, CNN, Nov. 15 2020
Faculty Senate Condemns COVID-19 Actions of Hoover’s Scott Atlas, Kate Chesley, Stanford News, Nov 20, 2020
Controversial White House Coronavirus Adviser Scott Atlas Resigns, Hallie Jackson and Tim Stelloh, NBC News, Dec 1, 2020
BIrx Confronted Pence About Atlas, Brett Samuels and Peter Sullivan, The Hill, Oct 19 2020
Debunking Denial: Ten False Narratives About the Coronavirus
Two Decades of Pandemic War Games Failed to Account for Donald Trump, Amy Maxmen and Jeff Tolleson, Nature Aug 4, 2020.
How many Needless COVID-19 Deaths Were Caused By Delays in Responding? Most of them. Isaac Sebenius and James K. Sebenius, STAT, June 19, 2020
Lockdown Delays Cost At Least 36,000 Lives, Data Show, James Glanz and Campbell Robertson, New York Times May 20, 2020
The Huge Cost of Waiting to Contain the Pandemic, Britta L. Jewell and Nicholas P. Jewell, New York Times Apr 14, 2020
How a Pandemic Might Play Out Under Trump, Ed Yong, The Atlantic, Dec 20, 2016
Take It From a Physician Treating COVID-19 Patients, ‘Frontline Doctors’ Video is Dangerous, Thomas Ken Lew, USA Today, Aug 3, 2020
‘I Happen To Think It Works:’ Trump Doubles Down on Hydroxychloroquine, Quint Forgey and Caitlin Oprysko, Politico July 28, 2020
Trump Health Aide Pushes Bizarre Conspiracies and Warns of Armed Revolt, Sharon LaFraniere, New York Times Sept 14, 2020
After Few Vaccine Reactions, Alaska Officials Stress That Reactions Are Treatable but COVID-19 is ‘Wild Card.’ Morgan Krakow, Anchorage Daily News, Dec 15, 2020.
Debunking Five Common Concerns About the COVID-19 Vaccines, Leana S. Wen, Washington Post, Dec 22 2020
Americans Increasingly Say They’ll Get COVID Vaccine, Ralph Ellis, WebMD, Dec 9, 2020
Anti-Vaccine Movement Could Undermine Efforts to End Coronavirus Pandemic, Researchers Warn, Philip Ball, Nature News May 13, 2020
Vaccine Opponents Outline Online Campaigns to Sow Distrust in Coronavirus Vaccine, Elizabeth Dwoskin, Washington Post, Dec. 23, 2020
COVID-19 Vaccines Face a Varied and Powerful Misinformation Movement Online, Brandy Zadrozny, NBC News, Nov 30, 2020
How a Kennedy Became a ‘Superspreader’ of Hoaxes on COVID-19, Vaccines, 5G and More, Alexei Mostrous, The Globe and Mail, Sept 16, 2020
Wikipedia, Robert Kennedy Jr.
Debunking Denial: Vaccinations
No, Robert F. Kennedy Jr is NOT a Vaccine Skeptic. He is a vaccine denier. And so is Donald Trump. Orac (David Gorski) Science blog, Jan 13, 2017
Clinical Outcomes in Young U.S. Adults Hospitalized with COVID-19, J.W. Cunningham et al., Journal of the AMA Sept 9, 2020; https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2770542
Is “Natural Immunity” from COVID Better Than a Vaccine? Apoorva Mandavilli, NY Times Dec 5 2020 https://www.nytimes.com/2020/12/05/health/covid-natural-immunity.html
Fewer than 1 in 10 Americans have antibodies to the coronavirus, https://med.stanford.edu/news/all-news/2020/09/few-americans-have-coronavirus-antibodies-study-finds.html
Wikipedia, Great Barrington Declaration, https://en.wikipedia.org/wiki/Great_Barrington_Declaration
Is Sweden’s Coronavirus Strategy a Cautionary Tale or a Success Story? Michael LePage, New Scientist Aug 13, 2020
Has Sweden’s Coronavirus Strategy Failed? Ishan Tharoor, Washington Post Nov. 18, 2020
Does Sweden’s COVID-19 Experience Support the Herd Immunity Theory? Arij Limam and Giulia Carbonaro, Newseu CGTN Nov 5, 2020
Sweden Has Become the World’s Cautionary Tale, Peter S. Goodman, New York Times July 7, 2020 (updated Dec. 15, 2020)
King of Sweden Blasts Country’s ‘Failed’ Coronavirus Response, Jon Henley, The Guardian Dec. 17, 2020
Analysis: Will Anyone Resign Over Sweden’s Coronavirus Strategy?, The Local (Sweden), Dec. 21, 2020
