
Controversies: Whether or not to Vaccinate
In Part I of this series, we gave a general summary of vaccination. Because the procedure of vaccination began in an attempt to provide immunity against smallpox, we provided a history of that disease and its effects. We first discussed inoculation techniques that pre-dated vaccination. Next we reviewed Edward Jenner’s introduction of vaccination, and the spread of this technique throughout the world. We also reviewed the concerted vaccination campaign that eventually led to the world-wide eradication of smallpox.
Next we reviewed poliomyelitis, the other disease that has been the subject of a major world-wide vaccination campaign. We now seem to be in the end-stage of the effort to eradicate polio. We introduced the concept of herd immunity, and discussed the relevance of this concept to vaccination campaigns. We ended with a brief summary of two other infectious diseases where vaccination has been effective, measles and mumps.
In Part II, we begin by reviewing the question “Should I vaccinate my children?” This is aimed at teenagers who may be reading this blog, or young adults who are just starting a family. Here we summarize the many benefits of vaccination to both individuals and to society. In the next section we review some of the controversies over vaccination from the 19th century, when the practice was first introduced and before the biomolecular basis of immunity was understood. In the final section of this part we review four discredited current myths regarding vaccination.
A. Should I Vaccinate My Children?
Our hope is that these posts are being read by teenagers and young adults, people who may soon have to choose whether or not to vaccinate their children. Our answer to them would be “By all means, vaccinate.” We hope that after you read these posts, it will be clear that vaccination is one of the greatest public-health benefits ever developed. As we showed, worldwide campaigns of vaccination have eradicated from the Earth one of the most deadly and disfiguring contagious diseases ever, smallpox; and we are close to eradicating polio. Furthermore, endemic measles has currently been eliminated in the U.S., and worldwide vaccination campaigns are decreasing every year the total number of measles deaths.
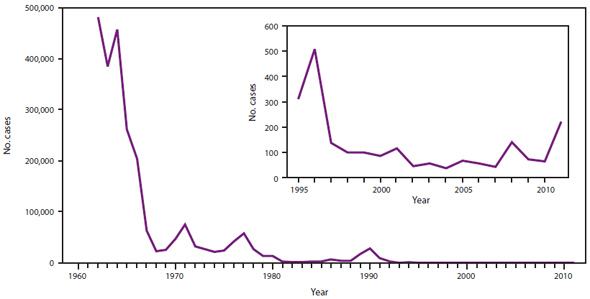
Let us try to answer some questions that readers may harbor regarding vaccination. First off, is vaccination really effective? The answer is definitely “Yes.” Figure 2.1 shows a graph of measles cases in the U.S. per year. At the start of a major vaccination campaign in the 60s, there were roughly 500,000 cases of measles per year. This sharply declined until in 1997 the number dropped to 100 per year or less. However, note that following 2007, measles cases in the U.S. again began to rise slightly. As we will see, this is a direct result of anti-vaccination campaigns aimed at the measles-mumps-rubella (MMR) combination vaccine. As we will show, such campaigns are based on misinformation. If vaccination rates of American children remain above 95%, measles cases should continue to decline, as is outlined in the section on “herd immunity” in part I of this series. Currently, endemic or “wild” cases of measles no longer occur in the U.S. Recent U.S. measles epidemics are the result of people becoming infected abroad, and returning to communities where the rates of vaccination are relatively low.
Other questions might be “Did you have your children vaccinated? Would you still repeat that today? And would you recommend that your grand-children be vaccinated?” The answer to all questions is “Yes.” As with all medical procedures, there are a few people who have adverse reactions to vaccines, but vaccination is generally quite a safe procedure, and the benefits to both the individual and society vastly outweigh the costs.
A third question would be whether one might avoid vaccinating one’s own children, and count on the remainder of the community to vaccinate their children, and thus protect one’s own family through herd immunity. After all, the risk of children contracting measles seems relatively low nowadays. But this is a risky and dangerous strategy, akin to Ruth Bader Ginsburg’s characterization of a majority Supreme Court decision as “like throwing away your umbrella in a rainstorm because you are not getting wet.” First off, you are protected from measles by herd immunity only if over 94% of the population is vaccinated. And even if 94% of the entire population is vaccinated, local groups with low vaccination rates could still be susceptible to a localized measles outbreak. This is apparently what happened with Amish groups in Ohio that suffered a measles epidemic in 2014.
Unfortunately, there is currently a lot of misinformation regarding vaccines. The biggest controversy is over claims that the MMR vaccine is associated with autism (see item #1 in section C below, “Myths About Vaccination”). This claim is primarily due to former British physician Andrew Wakefield (see C.1 in this part, and the entry on “Andrew Wakefield” in part III of this series). That claim has been completely disproved through extensive clinical trials all over the world. Similarly, various other negative statements about vaccination have been debunked, as we show in part C of this section.
Another myth is that multiple vaccines (particularly the MMR or MMRV shots) overwhelm or weaken an infant’s immune system (item #4 in Myths About Vaccination). This is one of the “explanations” that has been offered for the disproved “link” between the MMR vaccine and autism. Some anti-vaxers suggest that children should only get vaccinated for one disease at a time, and that vaccinations should be spaced out over time to avoid this “immune system stress.” This claim is addressed by Dr. Aaron Carroll, an expert on vaccination:
“Spacing out vaccines provides no benefit, and leaves children susceptible to illnesses for a longer time. It also requires more trips to the doctor, each of which is a chance to be exposed to other sick children. In addition, studies show that spacing out vaccines reduces the likelihood that children will complete the full schedule of immunizations.”
Or perhaps you will be persuaded by an outspoken defense of vaccination from a scientist and mother, and a critique of the anti-vaxer materials on the Web. We recommend Jennifer Raff’s blog post “Dear Parents, you are being lied to”. This post is filled with links to the medical literature. Thus you need not take the word of the author, you can go and read the relevant literature for yourself. And by the way, although much of the anti-vaxer materials urge you to “find out for yourself,” they generally provide links only to anti-vaxer claims and not to positive information about vaccination.
Finally, perhaps you will be convinced by video of an interview with Dr. Paul Offit, one of the most distinguished medical researchers on vaccines. Dr. Offit discusses recent controversies over vaccination, and his role in educating the public about the benefits of vaccination and the misinformation that is spread by anti-vaxers and their organizations.
Our aim is that young adults will realize that vaccination is the best hope for our society in fighting against a number of infectious diseases. We see that if nearly everyone has their children vaccinated, the benefits to society are dramatic; while once vaccination rates fall to a lower level, epidemics of preventable diseases will recur.
B. Early Controversies Over Vaccination
When vaccination was first introduced by Edward Jenner in about 1798, it is understandable that it would be controversial. First, at this time the germ theory of disease had not been fully articulated and studied, so the mechanism by which immunity was conferred through vaccination was not understood. Second, Jenner’s original method involved gathering material from individuals infected with cowpox, and then placing that material under the skin of another person.
So one could easily imagine that around 1800, the general populace would be very uneasy over the procedures suggested by Jenner. And indeed, there were very strong feelings among those doctors and scientists who advocated vaccination, and also by anti-vaccination groups that argued vociferously against the procedure.
Controversies over vaccination followed similar battles over the earlier practice of variolation. In part I of this series we mentioned that Rev. Cotton Mather had been a strong advocate of variolation in the American colonies. One of the opponents of this practice threw a home-made firebomb through the window of Mather’s house with an attached note that read “Mather, you dog, Damn you, I’ll inoculate you with this.” Luckily for Mather, the device failed to ignite.
And in Britain in 1772, Rev. Edmund Massey argued that preventing disease through variolation was a “diabolical operation.” Massey’s argument was that diseases were produced by God as a test of faith and also as punishment for sins. Thus, interventions by man to prevent disease would diminish the fear of God.
Below we show two cartoons that summarize the pro- and anti-vaccination camps, at the beginning of the 19th century. Figure 2.2 is an 1802 cartoon by James Gillray, titled “The Cow-Pock, or The Wonderful Effects of the New Inoculation.” The cartoon depicts a scene set at the Smallpox and Inoculation Hospital at St. Pancras, London. At far left, an assistant is ladling a liquid called “Opening Mixture” into the mouths of patients entering the doorway. To his right, Dr. Jenner (facing right) is shown injecting material into a lady’s arm, while a boy holds a pot of material labeled “Vaccine Pock Hot from Ye Cow.” To the right, the people receiving treatment are seen growing cows’ horns on their head, or sprouting heads of cows from various parts of their anatomy.

Initially I thought this poster was simply a clever satire on the use of pustules from cowpox in the vaccination procedure. However, I noted that the poster was published by “Ye Anti-Vaccination Society.” Upon further study, note that the painting on the back wall of the vaccination clinic depicts a crowd of worshippers paying homage to a statue of a golden calf.
Figure 2.3 shows a second cartoon, an 1808 illustration by Isaac Cruikshank. In this cartoon Dr. Jenner and two of his colleagues Thomas Dimsdale and George Rose (at right) are dismissing three anti-vaccination rabble-rousers, at left. A thankful mother sits in the middle background while babies who have apparently died from smallpox are shown in the foreground. The cartoon caption reads “Mercenary merciless spreaders of death and disease driven out of society.”

These two cartoons, the first of which is located at the British Museum and the second at the Wellcome Trust, give an indication of the ferocity of the debate on the merits of vaccination.
Figure 2.4 is a third cartoon, published in the 1880s by the London Society for the Abolition of Compulsory Vaccination. The paper held by the policeman reads “Vaccination Act for the Jenner-ation of Disease,” while the baby is being vaccinated by a skeleton. It should be remarked that one of the motivating factors behind the British anti-vaccination movement was the punitive effect on the poor. As part of Britain’s 1871 Vaccination Act, those who failed to have their children vaccinated could “face fines, confiscation of property or the workhouse,” according to Arthur Allen.

Let us briefly review some of the anti-vaccination arguments when the technique was first being employed. Objections based on religion were common. One objection was that no references to vaccination or similar procedures could be found in the Bible; the argument was that if God had intended man to utilize this technique, it would be mentioned in the Bible. Another argument was that vaccination could cause people to doubt God’s omnipotence.
Another objection was that the vaccination procedure involved injecting material into humans, which was deemed “unnatural.” The fact that the injected material was “foreign” (derived from another individual, a person suffering from a disease, and moreover the material was taken from pustules produced by an infected individual) was similarly viewed as morally objectionable.
Initially, the medical community itself was deeply divided regarding vaccination. One reason was that in the early days, matter from pustules that was used in the vaccination procedure could be contaminated by the smallpox virus. Thus, early instances of vaccination still produced an occasional case of full-blown smallpox. This was particularly troubling since the mechanism of immunity was unknown.
However, it rapidly became clear that vaccination was nearly always successful. And smallpox was a truly terrible disease, with tremendously high fatality rates or hideous disfigurement. A majority of the medical community very rapidly concluded that vaccination was effective.
The late Stephen Hawking liked to say that “Science wins because it works.” That is, one can marshal whatever arguments one wants against science and technology, but a crucial reason for adopting the scientific method is its proven success. In a similar way, vaccination won because it worked. The benefits of vaccination were dramatic and obvious – one did not have to understand the mechanism of immunity to realize that vaccination protected against smallpox. The medical profession in the 19th century had carried out an early version of a cost-benefit analysis. The results were not even close – the benefits greatly outweighed the costs. By the late 20th century, with the aid of advanced genetic mapping techniques, the biomolecular mechanism for generating immunity via vaccination became well understood, as detailed in Part I of this series.
Vaccination quickly became adopted throughout Europe in the early 19th century. For example, by 1840 the British government had banned variolation, and was providing vaccination free of charge. Vaccination programs were adopted throughout Europe. This technique soon spread to the Americas, and in short order a number of European nations were mounting large-scale vaccination campaigns in their colonies.
Think of the success of vaccination with respect to smallpox. One of the most dreadful infectious diseases of all time, one that had killed hundreds of millions of people worldwide, has now been eradicated from the globe. The eradication of smallpox was accomplished using vaccination, coupled with a massive coordinated public-health campaign. We are now in a similar position with polio, a disease that is likely to be eradicated within our lifetime.
C. Myths About Vaccination
There is currently a great deal of information on the Web regarding vaccination. In particular, there is an unusual amount of misinformation regarding vaccination. The groups promulgating these notions have a variety of motives. In this section, we discuss four myths about vaccination, its efficiency, its safety and groups that claim causal links between vaccination and other diseases, particularly autism.
Part III of this series contains capsule biographies of leaders of the “anti-vaxer” movement. There is a certain amount of repetition between this section and the information about anti-vaxers in Part III.
1) Disproven Myth: Vaccination causes autism
This myth was mainly propagated by a single person, the former British physician Andrew Wakefield (see his bio in part III, “The Anti-Vaxers”). In 1998, Wakefield and twelve co-authors published a paper in The Lancet alleging a link between the MMR (measles-mumps-rubella) vaccine and the onset of behavioral symptoms that they claimed were characteristic of autism. Wakefield and his co-authors claimed that within a short period after MMR vaccination (in some cases, two weeks), otherwise normal children would manifest these behavioral symptoms and would thereafter develop autism.
Wakefield’s paper caused a sensation. In Britain, immunization rates following the Lancet article dropped from 92% to 73%. The effects in the U.S. were not as dramatic but were still noticeable. The Lancet paper also galvanized the medical community into action. The Wakefield paper involved only 12 patients; so a number of much larger vaccination trials were undertaken. Those studies, which by now include millions of patients, found no link between vaccines and autism, or between the MMR vaccine and incidence of bowel disease.
Major clinical trials have completely ruled out the conclusions of Wakefield’s study. According to Dr. Aaron Carroll [this is repeated in Part III of this series]:
“The most recent Cochrane systematic review of research on the MMR vaccine included six self-controlled case series studies, two ecological studies, one case crossover trial, five time series trials, 17 case-control studies, 27 cohort studies and five randomized controlled trials. More than 15 million children took part in this research. No one could find evidence that vaccines are associated with autism.
[The assertion of a link between vaccination and autism] … is one of the most studied subjects ever. [In 2015], a study was published in the Journal of the American Medical Association that looked at a cohort of about 100,000 children. All of them were followed from birth until they were 5 years old. Researchers once again looked at whether the MMR vaccine was associated with autism, and found that it was not. It wasn’t even found among children who had siblings with autism and who would therefore be at higher risk for the condition.”
In addition, autism rates continued to rise in areas where MMR vaccination rates were decreasing. Finally, in 1993 Japan decided to discontinue the MMR vaccine. Following that step there was no corresponding decrease in autism rates in Japan.
In 2004, British journalist Brian Deer made a number of allegations against Wakefield. One of these was that Wakefield had been paid £400,000 by lawyers who intended to file lawsuits against the vaccine manufacturers, and that some of the patients in the Wakefield study had been recruited by one of those lawyers. At this point, 10 of Wakefield’s 12 co-authors on The Lancet paper retracted their conclusions on that paper. Further analysis of that paper, and the patients in that study, concluded that the paper was not just wrong but was fraudulent.
The UK General Medical Council then held hearings regarding Dr. Wakefield’s conduct. In Jan. 2010, the GMC ruled that Wakefield had “failed in his duties as a responsible consultant“, “acted against the interests of his patients,” and acted “dishonestly and irresponsibly” in his research. Upon their recommendation, Wakefield was struck off the UK medical register. In Feb. 2010, The Lancet formally retracted Wakefield’s paper.
Wakefield has been in Austin, Texas since 2004. After losing his medical license in the UK, he continues to maintain that there is a link between vaccination and autism. He is a major figure in U.S. anti-vaccination efforts, and he advises autism support groups that claim such a link.
In 2016, Wakefield directed a propaganda film Vaxxed: From Cover-Up to Catastrophe. Dr Ian Lipkin, professor of epidemiology and director of the Center for Infection and Immunity at Columbia University’s Mailman School of Public Health, wrote in a Wall Street Journal op-ed column: “Vaxxed … misrepresents what science knows about autism, undermines public confidence in the safety and efficacy of vaccines, and attacks the integrity of legitimate scientists and public-health officials.”
To summarize: from a study with 12 patients, Wakefield and his collaborators made sweeping allegations that the MMR vaccine was associated with the development of autism. Further studies of vaccination, now involving millions of children in many different countries, rebut Wakefield’s conclusions. (For additional details see the discussion of Wakefield in Part III).
2) Disproven Myth: Trace amounts of mercury in childhood vaccines are associated with medical issues, perhaps autism
Following Wakefield’s paper, a number of people have attempted to provide a scientific “explanation” for a purported link between vaccines and autism (remember, Wakefield’s “results” have been refuted). A common claim is that mercury compounds, particularly thimoseral, which was found in trace amounts in various vaccines, may be responsible for a number of adverse reactions that are perhaps connected to autism. Thimoseral is an organomercury compound that was a well-established antifungal and antiseptic agent. The purpose of thimoseral was as a preservative for the vaccines, to prevent contamination of the vaccine with fungi or bacteria.
It is important to point out that thimoseral was never an ingredient in the MMR vaccine. Therefore, claims that thimoseral in vaccines can cause autism cannot be related to Wakefield’s claim that the MMR vaccine could be implicated in causing autism. Claims regarding thimoseral are more likely to refer to vaccines that are given to infants, such as diphtheria or pertussis.
It is certainly true that exposure to high levels of mercury can cause serious neurological illness or death. The most widely-known case was that of residents of Minamata, Japan, where about 600 people died as a result of industrial methylmercury discharges into rivers and coastal waters. But it is important to note that thimoseral degrades into ethylmercury. The form of mercury that has been studied for its toxic effects is methylmercury, which has very different properties from ethylmercury. For example, methylmercury is actively transported across the blood-brain barrier while ethylmercury is not, so methylmercury is much more likely to cause neurotoxicity. In addition, there is evidence that ethylmercury in infants gets excreted in waste products.
The U.S. Food and Drug Administration has published a long discussion on thimoseral and its use in vaccines. Here we will summarize some of the results from that article.
After reviewing the data on thimoseral, the World Health Organization concluded that “there is currently no evidence of mercury toxicity in infants, children or adults” exposed to thimoseral through vaccination. Nevertheless, in 1999 the Centers for Disease Control and the American Academy of Pediatrics requested that vaccine manufacturers remove thimoseral from vaccines as a precautionary measure. This was rapidly accomplished in both the U.S. and the European Union. Since then, extensive studies in Denmark and Canada have shown that rates of autism continued to rise, even after thimoseral was removed from vaccines. Vaccines for children now contain either no thimoseral or trace amounts. And remember that the MMR vaccine never had any thimoseral.
Robert F. Kennedy Jr. has made strident claims that vaccines produce a number of adverse reactions in children, and that this is due to the presence of thimoseral in the vaccine. Kennedy’s claims contradict everything we know from comprehensive studies of vaccination and autism. The Institute of Medicine, the World Health Organization, the CDC and the FDA all reject any causal link between thimoseral and the incidence of autism. Nevertheless, it continues to be an article of faith among many anti-vaxer groups that vaccination is a cause of autism. And many of these groups attribute this to mercury compounds, particularly thimoseral, that have long since been removed from vaccines given to children in the U.S. or the European Union.
3) Disproven Myth: The Amish don’t vaccinate, and their children are essentially free from disease.
Several viral (not a pun) online posts make these claims, for example this one. This is an example of “New Age” myth. The crux of the article is that Amish children are generally not vaccinated, and that they suffer almost no diseases. This article claims that another “reason” for lack of disease in Amish children is that they don’t eat genetically-modified foods.
All of the claims in this article are false. First, a study of families in Holmes County, Ohio (which has a large number of Amish) showed that 85% of families had at least one child that had been vaccinated. Second, some Amish farms use genetically-modified crops for reasons of finance and efficiency. Third, not only do Amish children get sick, but they get some very serious diseases.
One of those is Maple Syrup Urine Disease, or MSUD. People with MSUD tend to experience vomiting, seizures and brain damage starting in infancy, and their life expectancy is quite low. Only 1 in 180,000 babies in the general population is born with MSUD, but in Amish communities the incidence is one in every 358 babies. The reason is that nearly all Amish in the U.S. can trace their lineage back to a few hundred Swiss farmers who immigrated in the 18th century. Several generations of inbreeding have left the Amish subject to these genetic-linked diseases.
The Amish make up 10% of the population of Geauga County, Ohio, but half of the special-needs children there are Amish. Several of these diseases appear to be genetic abnormalities resulting from the pattern of intermarriage in that community.
Finally, the notion that the Amish don’t get measles is simply wrong. Even though a significant percentage of Amish families have their children vaccinated, we know that measles will die out only if at least 94% of the population is vaccinated (see the discussion on herd immunity in part I). When the percentage who are vaccinated drops below that level, outbreaks of measles are likely to occur. Indeed, in 2014 a measles outbreak occurred in Ohio. The virus spread quickly in Amish communities where a relatively small number of children had been vaccinated. As a result, the Amish have been re-evaluating their practices with respect to vaccination.
It is true that the Amish have low incidence of some diseases, in particular various types of cancers. The Amish do not drink or smoke, and their long-sleeved clothing and wide-brimmed hats or bonnets protect them against skin cancer.
4) Disproven Myth: Vaccination against several diseases at once puts too much stress on an infant’s immune system.
This is another proposed “explanation” for the non-existent link between vaccination and autism. The argument is that shots such as MMR or MMRV that simultaneously vaccinate against several diseases are too stressful for an infant, and that the stress on the immune system leads to autism. This argument is bogus. As pointed out by Aaron Carroll, “Vaccines do not stress the human body that much. Children are continuously exposed to foreign substances that activate their immune systems. In a manuscript published in Pediatrics in 2002, Dr. Paul Offit and colleagues estimated that infants could respond to about 10,000 vaccines at any one time. The ones we give could never “use up” the immune system. It is thought that 11 vaccines at once might require the attention of about 0.1 percent of the immune system.”
Furthermore, studies show that children respond to multiple vaccines given simultaneously in a manner very similar to the response when vaccines are delivered one at a time. Vaccinated children are not at greater risk of infection from other pathogens than unvaccinated children. On the contrary, a German study of 496 children found that children who received vaccinations against multiple diseases within the first 3 months of life had fewer infections from either vaccine-related or unrelated pathogens than unvaccinated children.
Carroll’s article concludes, “Current studies do not support the hypothesis that multiple vaccines overwhelm, weaken or “use up” the immune system. By providing protection against a number of bacterial and viral pathogens, vaccines prevent the “weakening” of the immune system and consequent secondary bacterial infections occasionally caused by natural infection.”
President Trump appears to subscribe to the theory that multiple vaccines place too much stress on an infant’s immune system and lead to complications. We review Trump’s comments on this issue in Part III of this series.
D. Vaccination in the U.S.: State Regulation of Vaccination
Once the mechanism of vaccination and the acquisition of immunity was understood, the next issue was for society to determine which individuals should be vaccinated. Governments view vaccination as an obvious benefit to society. Vaccinating children confers immunity upon them. After vaccination, individuals benefit from greater health and they are not exposed to suffering a preventable disease. Society is subsequently freed from the expense of providing hospitals and care for people who catch the disease.
According to the World Health Organization (WHO), the most common and serious vaccine-preventable diseases are: diphtheria, Haemophilus influenzae serotype b infection, hepatitis B, measles, meningitis, mumps, pertussis, poliomyelitis, rubella, tetanus, tuberculosis, and yellow fever. In addition, WHO lists 25 diseases for which effective vaccines are available. We discussed polio and the polio vaccine at significant length in Part I of this series. Here, we will focus on the measles-mumps-rubella combination vaccine (MMR), in part because it is the most common childhood vaccine and partly because it has become the most controversial. New vaccines frequently combine the MMR vaccine with one against varicella or chicken-pox.
In the U.S. today, the question of who should be vaccinated remains controversial. The requirements for vaccination are left to individual states. At present, all 50 states require that parents vaccinate their children against a variety of diseases, generally measles, rubella and polio (and sometimes mumps and chickenpox) as a condition of enrollment in public schools.
One class of children are uniformly exempted from the requirement of vaccination, and that is medical exemptions – for children who are allergic to vaccines, have compromised immune systems or are otherwise in poor health.
The Supreme Court has affirmed a state’s right to compulsory immunization requirements, on the grounds that the state’s interest in promoting communal safety overrides an individual’s liberty to opt out of vaccination. In Prince v. Massachusetts (1944), the Supreme Court stated: “The right to practice religion freely does not include liberty to expose the community or the child to communicable disease or the latter to ill health or death … Parents may be free to become martyrs themselves. But it does not follow [that] they are free, in identical circumstances, to make martyrs of their children before they have reached the age of full and legal discretion when they can make that choice for themselves.”
However, after the Supreme Court ruling affirming that states can compel individuals to vaccinate their children, most states have carved out additional exemptions based on either religious or philosophical beliefs. The National Conference of State Legislatures has published a guide that discusses the non-medical exemptions that states allow for vaccination. This is summarized in Fig. 2.5 below.
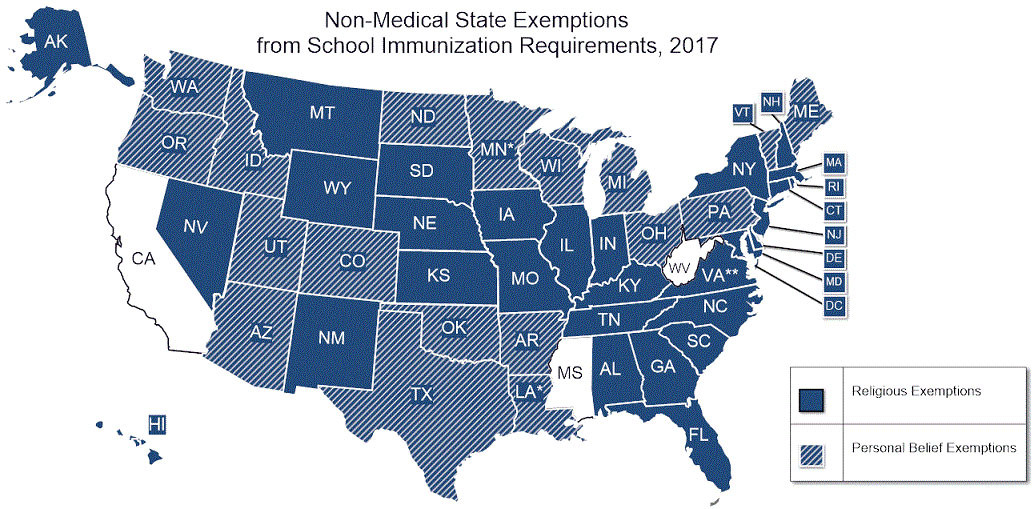
Figure 2.5 shows that 47 states allow non-medical exemptions for vaccination (the existing statutes in Louisiana and Minnesota do not explicitly recognize religion as a ground for obtaining an exemption, but in practice those states allow exemptions based on religious belief). Only West Virginia and Mississippi do not allow exemptions on the basis of either religious or philosophical beliefs. In 2015, California removed exemptions based on personal beliefs, and the language in that bill includes religion under the category of personal belief.
Another 18 states allow exemptions from vaccination for both personal and religious beliefs. In recent years, following a number of well-publicized outbreaks of infectious diseases, several of which were linked to religious communities that tended not to vaccinate their children, a number of states have attempted to limit the number of people who obtain non-medical exemptions. A few states have amended their laws so that non-vaccinated children (who were exempt from the vaccination requirement) can be held out of school in the event of an outbreak.
The states are attempting a delicate balancing act. From a public-health perspective, the number of children being vaccinated should be as high as possible. States also desire to provide some accommodation for people who do not want their children vaccinated. This is particularly true for religious beliefs, since organized religion plays such a prominent role in American society.
Some commentators have pointed out that states which allow exemptions from vaccination requirements for religious beliefs, but not for other philosophical reasons, may face legal challenges to their statutes. Courts could rule that those states are illegally favoring certain moral beliefs over others. Ciolli (Missouri Law Review 74, article 3 (2009)) makes the interesting suggestion that states could provide non-medical exemptions, but charge those parents a fee for the exemption. The proceeds from this fee would be deposited into a fund used to defray the expenses resulting from epidemics of infectious diseases among non-vaccinated children. The fee would quite likely turn out to be significant.
In recent years we have seen substantial increases in the number of Americans who fail to have their children vaccinated. There have been two major incidents that raised concerns that vaccination might have significant adverse effects. We have discussed the second of these, Andrew Wakefield’s now-discredited 1998 paper alleging a link between the MMR vaccine and autism.
An earlier event was a 1982 TV documentary called DPT: Vaccine Roulette, that was produced by journalist Lea Thompson and aired by a Washington, D.C. NBC affiliate. Thompson’s documentary focused on the vaccine for pertussis (or whooping cough, the “P” in the DPT or diphtheria-pertussis-tetanus vaccine given to newborns). Thompson was an award-winning investigative journalist; however, she was not a scientist.
DPT: Vaccine Roulette was compelling television. Seth Mnookin describes Thompson’s documentary as “an example of scare-mongering at its worst: Throughout the hour-long show, Thompson featured heart-breaking interviews with parents who described how their children had been left in near-comatose states after receiving a vaccine that was mandatory for public-school children in the vast majority of states. These were augmented by what turned out to be inaccurate statistics, cherry-picked quotes, and risible falsehoods about some of the ‘experts’ Thompson used to support her thesis that the ‘medical establishment’ was ‘aggressively promot[ing]’ a vaccine while willfully ignoring ‘the consequences.'”
Thompson’s documentary had a number of dramatic effects. The pertussis vaccine was a “whole-cell” formulation consisting of killed pertussis cells. This vaccine did have a number of side effects, although scientists reject Thompson’s claims that the vaccine was responsible for the severely brain-damaged children shown in her documentary. The medical community maintains that the cause of those children’s disability was infantile epilepsy. In 1990, the Journal of the American Medical Association called the connection a “myth” and “nonsense.”
Nevertheless, in 1992 an acellular version of the pertussis vaccine was approved for use in the U.S. This version is part of the DTaP (Diphtheria-Tetanus-acellular Pertussis) vaccine now in use in the U.S. The acellular pertussis vaccine has a significantly lower rate of adverse side effects, although it appears that it may be slightly less effective against whooping cough than its predecessor.
Thompson’s documentary led to serious concerns among the general public. Her documentary was the inspiration for some of the modern American anti-vaccination groups. Barbara Loe Fisher co-founded the anti-vaxer organization The National Vaccine Information Center after watching DPT: Vaccine Roulette.
Following the documentary, vaccination rates went down in the U.S., cases of whooping cough went up, and lawsuits against vaccine manufacturers increased dramatically. The price of the DPT vaccine increased dramatically, and by the end of 1985 only one manufacturer remained in the U.S.
As a result, in 1986 Congress passed the National Childhood Vaccine Injury Act. This established a federal system to compensate victims of injury that resulted from mandatory vaccinations. Claims are reviewed by a review body colloquially called the “vaccine court,” and awards are made if the claim is deemed to have merit.
At the same time, the U.S. government set up systems that were capable of alerting physicians and manufacturers to possible adverse effects. The CDC and FDA jointly established the Vaccine Adverse Event Reporting System (VAERS). Anyone can report suspected adverse reactions from vaccination through this system. In addition, the Vaccine Safety Datalink system collects all vaccine-related information from a number of large health providers.
Aaron Rothstein’s review of vaccine controversies proposes a link between modern anti-vaccination efforts and the growth of feminism and patients’ rights groups. Rothstein notes the connection to a cultural reaction against medical paternalism. He states that: “alongside a growing emphasis on patient autonomy, we have seen greater respect afforded to the views of women and mothers, as well as trends toward the wider dissemination of scientific information, and toward a broader questioning of reductionist science by the environmental movement. To some extent these are salutary reactions against paternalism, sexism, and technocracy, but they have at times also led to the propagation of irrational fears and the embrace of quackery.”
Indeed, much early research on vaccines employed methods that would never be countenanced today. For example, Rothstein reports that “many of those whose research laid the foundations for modern vaccines, such as Jonas Salk, Maurice Hilleman, and Stanley Plotkin, tested their vaccines on mentally retarded children. Starting in the mid-1950s and continuing for about fifteen years, the infectious-disease doctor Saul Krugman fed hepatitis virus to severely disabled residents of the Willowbrook State School in order to study the virus.”
The modern anti-vaxer movement is connected to what many see as an over-reaction to the authority of doctors and scientists. Elena Conis, author of the 2014 book Vaccine Nation, states that “Health feminists cultivated the notion that knowledge gained through personal experience was just as valuable or even more valuable than medical knowledge.” Conis quotes a chiropractor as claiming that “there is a wisdom within the body … has the most complex organic machinery in the world. It produces all the chemicals one will ever need to be healthy…. The wisdom that created our bodies is far superior to the finite mind of all the scientists in the world.” Given such a worldview, vaccines would be viewed as both unnatural and unnecessary.
In Part III of this series our discussion of leading anti-vaxers includes actress and activist Jenny McCarthy. In a 2007 appearance on the Oprah Winfrey show, Ms. McCarthy responded to experts from the CDC who claimed that science clearly demonstrated that vaccines do not cause autism. McCarthy asserted that “my science is named Evan [her son], and he’s at home. That’s my science.” She also asserted that her “mommy instinct” allowed her to “know what’s going on in his body.”
