
April 24, 2024
I. Background
In June 2022 in the case Dobbs v. Jackson Women’s Health Organization, the U.S. Supreme Court overturned its own 49-year-old Roe v. Wade precedent regarding a constitutional right for women to seek abortion up until the point of fetal viability. In the majority Dobbs opinion, Justice Samuel Alito took pains to assure that “Nothing in this opinion should be understood to cast doubt on precedents that do not concern abortion.” However, Justice Clarence Thomas did his best to undermine that assurance in his concurring opinion, writing that since the Court had now gotten abortion law right, the Justices “should reconsider all of this Court’s substantive due process precedents, including Griswold, Lawrence, and Obergefell,” three other cases that the dissenting Justices described as “all part of the same constitutional fabric protecting autonomous decision making over the most personal of life decisions.”
In particular, the 1965 case Griswold v. Connecticut had produced a Supreme Court ruling that “the Constitution did in fact protect the right of marital privacy against state restrictions on contraception.” The Court ruled in that case that a right to privacy in marital relations was indirectly guaranteed by the combination of the First, Third, Fourth, and Ninth Amendments to the Constitution. Concurring Justices cited instead the Ninth and Fourteenth Amendments, in particular the Due Process Clause of the latter. The Court later extended constitutional protections for contraception to unmarried people in the 1972 case Eisenstadt v. Baird.
Justice Thomas’ Dobbs opinion confirmed that he had well absorbed the Christian Nationalist-tinged training in conservative law interpretation offered for decades by the Federalist Society, under the leadership of Leonard Leo. With regard to contraception, in particular, the efficacy of that training was highlighted in a 2023 New York Times op-ed written in the light of Congressional Republicans blocking a bill to enshrine a federal right to contraception and the decision by the Food and Drug Administration (FDA) to approve for sale the first over-the-counter birth control pill, the Opill (see Fig. I.1). In the op-ed Hadley Heath Manning, a staffer for Independent Women’s Voice and Independent Women’s Forum, explained that “Conservatives generally see birth control as…a personal choice,” rather than as a “positive right” worthy of legal protection. The problem with that view is that without a law guaranteeing access to contraception and with a Supreme Court willing to entertain the prospect of overturning Griswold, there is a real possibility that states will pass laws to restrict access to contraception or even to remove the option of that personal choice, just as they have already done with regard to abortion in the wake of the Dobbs decision.

On the other hand, Republican-controlled state legislatures may be hesitant now to pass laws restricting contraception after seeing how widespread and long-lasting the political backlash has been to the rash of state laws severely restricting abortion in the immediate wake of the Dobbs decision (see the map in Fig. I.2). Many states have banned all abortions or banned abortions after the 6th week of pregnancy, by which point many women do not yet know for sure that they are pregnant. In some states, there are no exceptions allowed for rape or incest. Furthermore, language regarding the health of the mother is sometimes so ambiguous that physicians are reluctant to carry out any procedures that might be interpreted as abortion even when the mother’s life is clearly jeopardized.

In response to this swift anti-abortion wave, voters have reacted strongly and negatively. Republicans did much worse than had been expected in the 2022 midterm elections and in special elections held since then. A number of states have adopted by large voting margins citizen-initiated referendums placing (or not replacing) abortion protections in state constitutions, including in such conservative states as Kansas, Kentucky, and Ohio. Similar referendums may be on the ballot in up to 11 additional states for the 2024 Presidential election. And there is no evidence that the uproar has abated since the Dobbs decision.
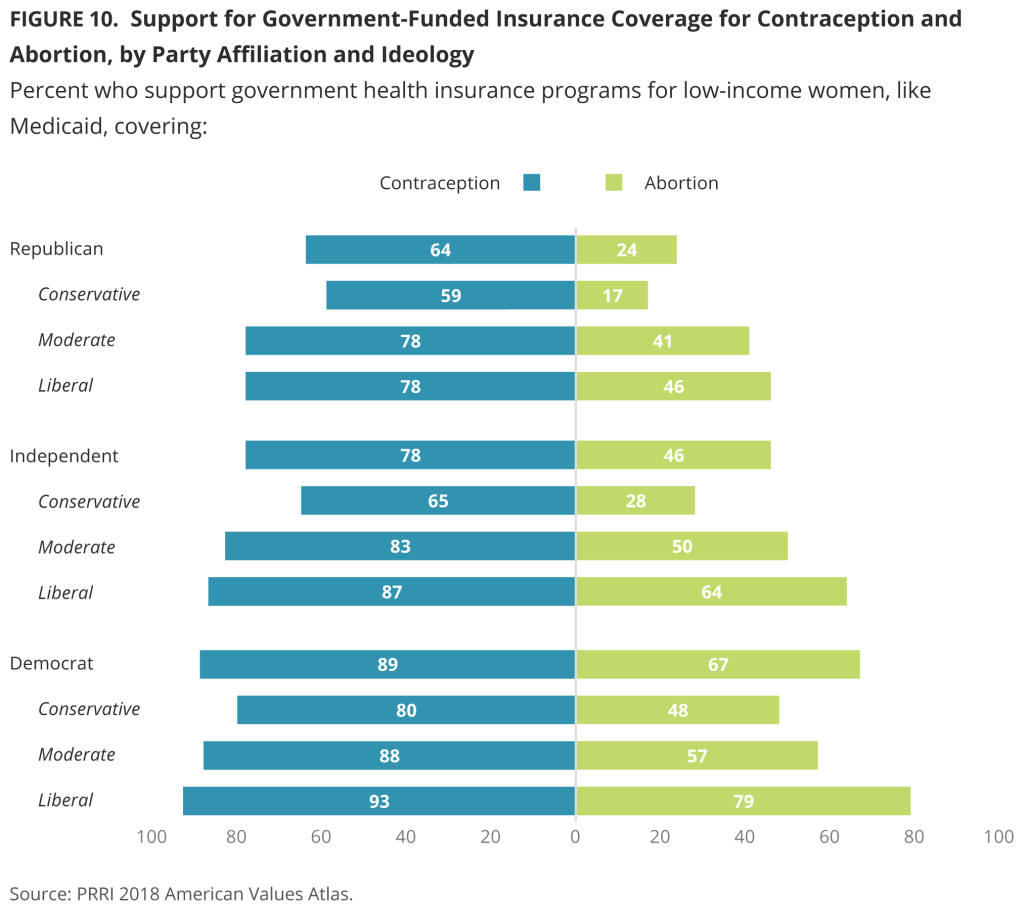
The political backlash would be even much stronger to any attempt to legalize restrictions of access to contraceptives. As indicated by the survey results in Fig. I.3, U.S. citizens of all political leanings strongly support not only access to contraception, but even government-funded insurance coverage for contraception. The vast majority of American families rely on contraception in some form to limit family size. It is unlikely that Republican-controlled state legislatures or the U.S. Congress will take the political risk of legislating against that strength of public opinion, despite pressure from Christian Nationalist groups.
In fact, opposition to contraceptives is the subject of a religious, as well as a political, controversy. Following the release of oral contraceptives in 1960, the Catholic Church under Pope John XXIII established a Pontifical Commission on Birth Control, to reconsider a ruling in 1930 that prohibited contraception. Pope Paul VI expanded the commission to 64 members; they issued a report recommending that the church approve of artificial contraception, without distinguishing between various methods. A minority of 4 members of the commission opposed that recommendation. However, Pope Paul VI issued an encyclical in July 1968 that reaffirmed the Catholic Church’s prohibition on artificial contraception. One of the arguments was that a primary goal of sexual relations was for the purpose of conceiving children and that sex must necessarily be “open to the transmission of life.” The encyclical of Paul VI, particularly since it directly contradicted the recommendations of a great majority of his own commission, made this report unusually contentious. Several bishops and cardinals spoke out against the prohibition of contraceptives. Such open opposition to a manifesto of the Church was almost unheard of.
Immediately following the release of the encyclical, a group of American dissident theologians issued a statement that “spouses may responsibly decide according to their conscience that artificial contraception in some circumstances is permissible.” And the Canadian Conference of Catholic Bishops stated that “those who cannot accept the teaching should not be considered shut off from the Catholic Church.” In 2011 the Guttmacher Institute released the results of a study of American women of reproductive age who had ever had sex. They found that 99% of these women had used a method of contraception other than natural family planning. This group included 98% of those who identified as Catholic women. Thus, the papal encyclical on contraception has been almost universally disregarded by American Catholics. As a result, in recent decades the Catholic Church in America has not emphasized its opposition to artificial contraceptives, since this edict is overwhelmingly ignored by its members. However, as laws restricting abortion have been passed in many states following the Supreme Court’s Dobbs decision, it may only be a matter of time before Catholic Church officials begin to stress the Church’s opposition to contraceptives, and to apply pressure on its members to cease using contraceptives.
In the light of the religious controversy and the strong popular opposition, what’s a Christian Nationalist to do? They have undertaken since the Dobbs decision, and more strongly in the wake of the FDA approval of Opill, a disinformation campaign targeting teenage and young women on their preferred social media platforms, TikTok and Instagram. They spread myths about the negative health and social impacts of hormonal contraception – particularly, birth control pills and intrauterine devices (IUDs) – trying to create a generation of women who abandon these methods. Instead, they promote natural family planning, or fertility awareness – what used to be called the Rhythm Method of avoiding unprotected sex before and during the estimated ovulation period. But now those methods are supported by smart phone apps that help to identify “ovulation week” for users via their bodily measurements, so the method today would be better labeled as “algoRhythm.”
Their opposition to “non-natural” contraception creates a credibility problem for many anti-abortion activists. There is considerable research and experience worldwide to demonstrate that providing access to modern contraceptives is the most effective way of reducing the rate of abortions. We will review that evidence in Section II of this post. Even conservative Hadley Heath Manning in the op-ed referenced above admits that “many Americans who oppose abortion see preventive birth control as a tool to reduce the demand for it in the first place.” So, how can one claim to oppose abortion out of concern for the life of the unborn child and at the same time oppose preventive birth control that effectively reduces abortions? We will speculate on the hidden agendas behind this conundrum in Section V of this post, after first describing the ongoing disinformation campaign in Section III and comparing the action and efficacy of fertility awareness vs. hormonal contraceptive methods in Section IV.
Many activists try to wriggle out of this credibility dilemma by purposely obfuscating the distinction between contraception and abortion. For example, “Dr. Ingrid Skop, the director for medical affairs at Susan B. Anthony Pro-Life America’s research arm called the Charlotte Lozier Institute… claimed that there are safety concerns with Opill as an “abortifacient,” i.e., a pharmaceutical method for effecting an abortion. The main action of birth control pills is to suppress ovulation. If there is no egg released from the ovaries to fertilize, there can be no conceivable “beginning of life.” The birth control pills also induce other alterations of the uterus and the passageway to it in order to suppress fertilization even if an egg is accidentally released.
The conflation of abortion and contraception is a central aspect of the “personhood” movement, in which many anti-abortion activists are pressuring states to pass laws identifying fertilized eggs (even when not implanted in the uterus), embryos, and fetuses as “persons” with all the same rights as those already born. Personhood goes well beyond the existing U.S. legal definition of pregnancy as beginning when a fertilized egg is implanted in a woman’s uterus. That definition allows for the medical fact (to be discussed in Section V) that a sizable fraction of fertilized eggs fail to implant under natural conditions. But personhood implies, as revealed in a February 2024 Alabama Supreme Court ruling, that even spare frozen embryos created, but not implanted, in an in vitro fertilization (IVF) procedure, should be considered as unborn children. This ruling, if allowed to stand, would most likely imply that IVF is illegal because the frozen embryos might go unused or be inadvertently destroyed. But IVF is highly popular among people of all political persuasions as it provides a method to aid couples who have difficulty conceiving naturally. The political confusion of Republicans trying to navigate a path between pressure from the personhood proponents and upsetting large portions of the electorate was exemplified when Alabama Senator Tommy Tuberville was interviewed in the wake of the Alabama court ruling; within one minute the Senator went from “I was all for it” concerning the ruling that jeopardizes IVF to “I agree. People need to have access” to IVF, with a lot of word salad in between.
II. Access to contraception reduces the frequency of abortions
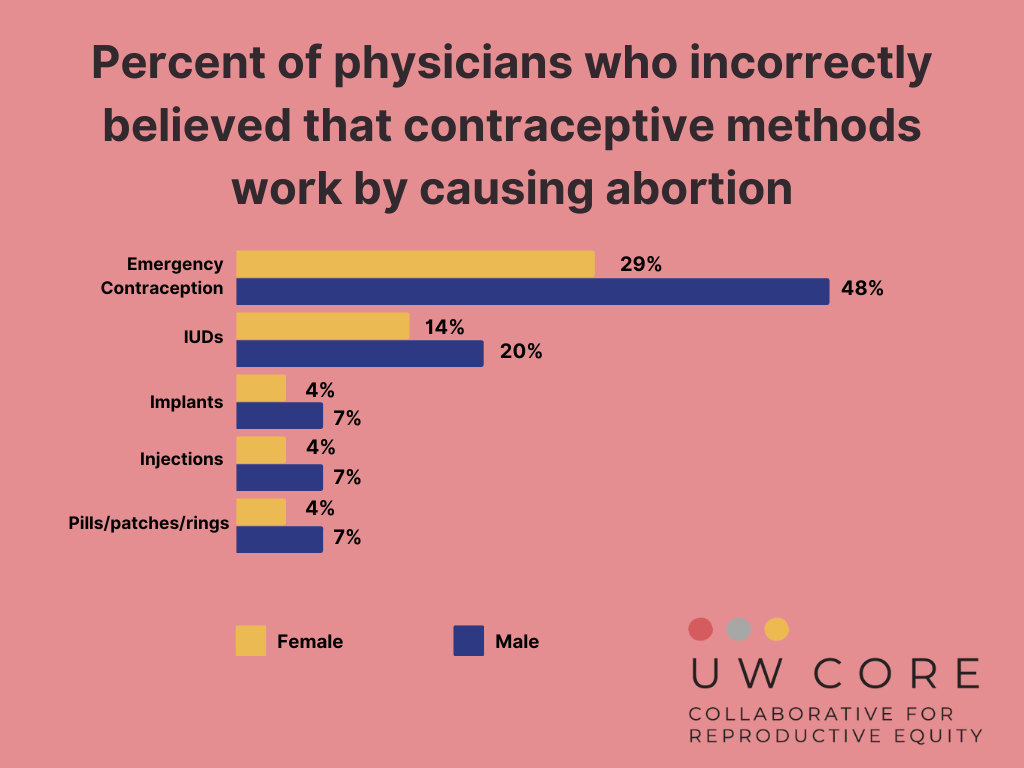
The distinction between contraception and abortion is clear if one accepts the U.S. legal definition (according to the Code of Federal Regulations, 45 CFR § 46.202) that pregnancy begins with the implantation of a fertilized egg in the uterus. Contraception is intended to prevent pregnancy while abortion is intended to terminate pregnancy. Despite widespread misunderstanding (which applies even to physicians, see Fig. II.1), this distinction applies as well to emergency contraception, such as Plan B, that is taken after unprotected intercourse, while sperm may still be active in the woman’s body. Plan B is still designed to suppress ovulation, not to terminate an initiated pregnancy. All forms of contraception are thus aimed (with varying efficacy) at preventing unintended pregnancies, while it is unintended pregnancies that often lead to abortions.
A 2020 article in The Lancet Global Health estimated the unintended pregnancy and abortion rates worldwide. The authors estimated that for the years 2015-19 “there were 121.0 million unintended pregnancies annually…corresponding to a global rate of 64 unintended pregnancies…per 1000 women aged 15–49 years. 61%…of unintended pregnancies ended in abortion…corresponding to a global abortion rate of 39 abortions…per 1000 women aged 15–49 years.” To turn that statistic around, a 2012 Brookings Institution study found that more than 90% of all U.S. abortions are due to unintended pregnancies. Figures II.2 and II.3 from The Lancet paper show that while the unintended pregnancy rate varies strongly with mean income within a country, the fraction of unintended pregnancies that end in abortion is high for all income groups and even in countries with restrictive abortion laws.


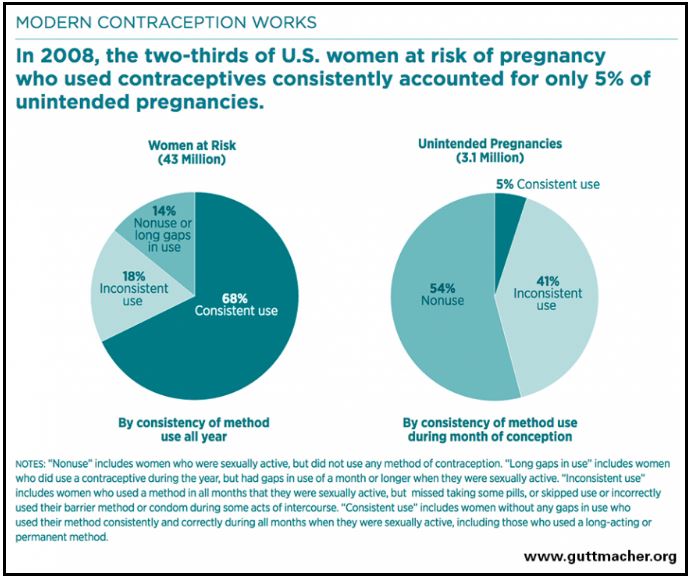
Although the rate of unintended pregnancies in the above figures is high, the trend in Fig. II.4 shows that it has been declining steadily worldwide for decades as the use of modern contraceptives has increased. There is an extensive amount of data demonstrating that providing free access to modern contraceptives is the key to reducing abortion rates. A Guttmacher Institute survey in 2008 revealed (Fig. II.5) that the 68% of U.S. women of childbearing age who used modern contraceptives consistently accounted for only 5% of all U.S. unintended pregnancies. Indeed, as contraceptive usage has expanded in the U.S., especially among young women, the abortion rate has dropped steadily since 1980 (see Fig. II.6) well before the Dobbs decision, a statistic one doesn’t often hear about in the social, political, and legal battles over abortion.


Access to contraceptives has had similar impacts on abortion rates in many countries. As examples, Figs. II.7 and II.8 present statistics from South Korea and from Shanghai, China. In South Korea following the Korean War of the early 1950s a high national birth rate doubled the population in 35 years. The economic boom that resulted from that Baby Boom was accompanied by a contraception boom and a precipitous decrease in fertility rates, down to the currently unsustainable level below 0.9 live childbirths per woman. But as contraceptive prevalence grew, the country’s abortion rate also dropped precipitously from a high of about two lifetime abortions per woman to a very low rate today.
In China the incidence of abortion was also influenced by the One-Child policy that was in effect from 1979 through 2015. Families that had a first child then avoided a second either by abortion or contraception. As the figure below shows, in the years following the first childbirth women’s use of an IUD for contraception gradually grew and as it did, the rate of abortions rapidly dropped.

If the correlations in the above figures don’t convince you of the efficacy of contraception in reducing abortion rates, consider the Contraceptive CHOICE Project carried out by medical researchers from Washington University, Saint Louis, from 2007 to 2011. The Project enrolled 9,256 women and adolescent girls (ages 14-45), both white and black, from the St. Louis area at risk for pregnancy. 97% of the participants were sexually experienced at the start of the Project, and that figure rose to 99% within a year. The Project leaders offered participants free birth control using a method of each participant’s choice: either long-acting birth control devices such as IUDs and implants, or shorter-acting methods such as birth control pills, patches and rings. Each participant was counseled on the usage, risks and benefits of each of the available methods. “When barriers to contraception such as cost and lack of education were removed, most [about 75%] teens in [the] Washington University study opted for long-acting birth control,” which didn’t require them to remember to take the pill every day.
Pregnancies, births, and abortions were monitored for every participant from 2008 to 2010. Overall, abortion rates dropped by between 62% and 78% compared to the relevant national U.S. rates and to the local rates within St. Louis county. The impact among adolescent girls is shown in Fig. II.9, where pregnancy and abortion rates for the teen participants are compared to national U.S. averages for sexually experienced teens. The rates for study participants were lower than the national averages by factors of 4—5.

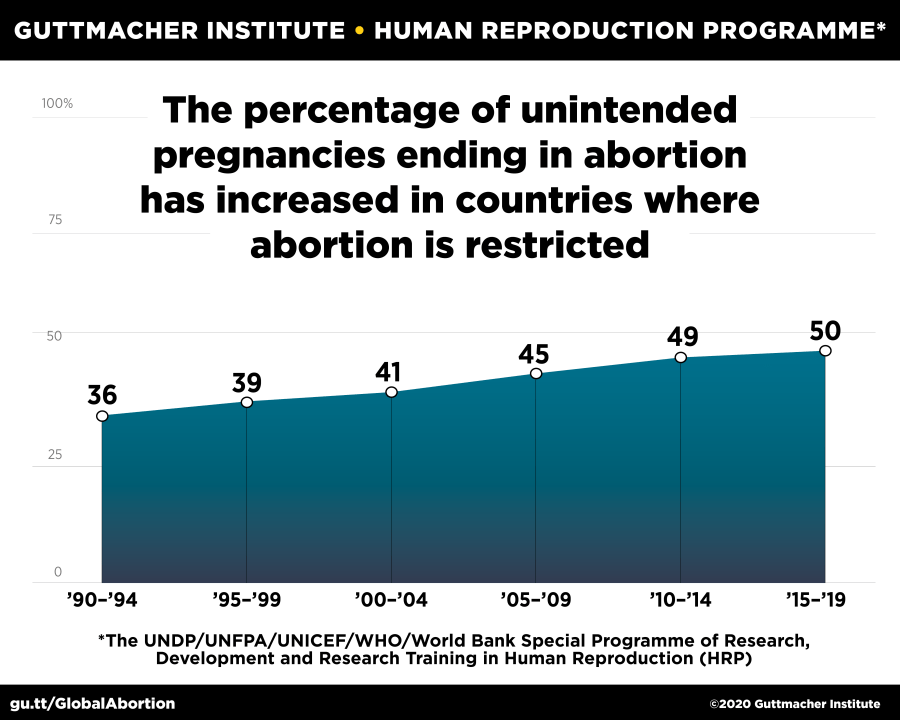
In light of the evidence it seems that anti-abortion activists who claim their passion is driven by concern for unborn children betray a hidden agenda (see Section V) when they also passionately oppose contraception, since contraception is the most direct way to reduce the incidence of abortion. The activists may believe that abortions would not increase if non-natural contraception methods were banned, because abortions will be made illegal. But the evidence from other countries does not support such a claim. Figure II.10 shows that even within countries where abortion is severely restricted (i.e., either completely prohibited or allowed only when the pregnancy poses great danger to the health or life of the mother), the percentage of unintended pregnancies ending in abortion has increased steadily throughout this century. If contraception access were restricted the rate of unintended pregnancies would greatly increase and abortions would rise, even if they have to be done by black market sale of abortifacients.
III. The disinformation campaign
As of now, access to contraceptives is a constitutionally guaranteed right in the U.S. in the wake of the Supreme Court’s decisions in Griswold v. Connecticut and Eisenstadt v. Baird. But Clarence Thomas’ concurring opinion in Dobbs has certainly created nervousness. A Right to Contraception Act was introduced in Congress in the aftermath of Dobbs, but was blocked from consideration by Senate Republicans. Thirteen U.S. states — California, Colorado, Florida, Illinois, Massachusetts, Michigan, Minnesota, New Jersey, New Mexico, Oregon, Rhode Island, Vermont, and Washington – plus the District of Columbia currently have either laws or constitutional clauses protecting the right to contraception. Florida is the only one of these that has also passed a restrictive abortion law. In addition, Maryland and Nevada will have upcoming ballot measures to add constitutional protections for contraceptive access. In the wake of Dobbs President Biden issued two executive orders providing some federal protection for access to reproductive health care, including contraceptives, but these could be overturned by a different President.
No U.S. state has yet tried to pass a law restricting access to contraception so that the issue could be reconsidered by the Supreme Court. There may, indeed, be reluctance to do so in light of the serious political backlash to the restrictive abortion laws passed (or revived) after Dobbs. However, given widespread misunderstanding among the public and many physicians regarding the distinctions between contraceptives and abortifacients, some of the restrictive state abortion bans may lead either to bans or at least ambiguity regarding specific types of contraception. The issue arises in states that have defined pregnancy, either explicitly or implicitly, to begin at fertilization rather than at implantation of a fertilized egg in the uterus. We will explain in Section V why such a legal definition is illogical.
Emergency contraceptives, such as Plan B, are widely misunderstood to terminate a pregnancy – in reality, they just suppress ovulation after intercourse, while sperm still survive within the woman’s body – while IUDs are widely misunderstood to work primarily by preventing implantation – in fact, they suppress access of sperm to reach eggs. These misunderstandings may certainly impede doctors in some restrictive abortion states from prescribing either IUDs or emergency contraceptives (which are essential, for example, in cases of rape). At the very least, some states have barred emergency contraceptives from being covered by state Medicaid plans.
With limited hopes on the legal front, opponents of contraception have engaged in a disinformation campaign on social media, a campaign that has kicked into high gear since the FDA in July 2023 approved the first over-the-counter birth control pill – Opill – for sale without the need for a prescription. Opill became available for online sales in mid-March 2024. The disinformation campaign is being waged primarily on TikTok and Instagram, platforms used preferentially by teenage and young women, a group that accounted for about one third of global sales of hormonal contraceptives in 2022. Messages warn of dangers to a woman’s health and social well-being from the use of hormonal contraceptives. Young women who seem receptive to these false messages are then sent many of them by the social media algorithms that promote confirmation bias. The onslaught of such messages reinforcing misinformation is given more credence than scientific evidence by some young women.
The onslaught of posts claim that birth control pills cause weight gain, anxiety, depression, low libido, infertility, several mental health problems, increased susceptibility to sexually transmitted infections, and other horrors. A recent Washington Post article gives some specific examples. “Brett Cooper, a media commentator for the conservative Daily Wire, argued in a viral TikTok clip that birth control can impact fertility, cause women to gain weight and even alter whom they are attracted to. It racked up over 219,000 ‘likes’ before TikTok removed it following The Post’s inquiry… Cooper and political commentator Candace Owens denounce birth-control pills and IUDs as ‘unnatural,’ with Owens saying she’s a ‘big advocate of getting women to realize this stuff is not normal’… On his show, Ben Shapiro, another right-wing pundit, called discussing birth-control side effects a ‘political third rail,’ while interviewing a guest who proclaimed that women on birth-control pills are attracted to men who are ‘less traditionally masculine.’” There is some scientific evidence that hormonal contraceptives may change women’s preference for male scents, but characterizing that as a preference for “less traditionally masculine” men is purposely provocative. Another example from the Washington Post article: “The online magazine Evie, described by Rolling Stone as the conservative Gen Z’s version of Cosmo, urges readers to ditch hormonal birth control with headlines such as ‘Why Are So Many Feminists Silent About The Very Real Dangers Of Birth Control?’” In addition, “Celebrities including Dr. Oz, Gwyneth Paltrow, and podcaster Joe Rogan have all promoted the idea that hormonal birth control is unwholesome and potentially dangerous.” We have previously profiled the first two of these celebrities in our (unflattering) posts on Wellness Fads.
Other anti-abortion activists have purposely conflated contraception and abortion. As we noted earlier, Dr. Ingrid Skop of Susan B. Anthony Pro-Life America has claimed that there are safety concerns with Opill as an “abortifacient,” even though it is nothing of the sort. In the wake of the FDA’s Opill decision, Emma Posey Waters of the Independent Women’s Forum and the Heritage Foundation has spread disinformation that “increased access to birth control leads to increased abortions,” while the evidence we have summarized above demonstrates exactly the opposite. The anti-abortion group Students for Life of America (SFLA), for whom Leonard Leo serves as co-chair of the Board, has asserted that allowing over-the-counter access to Opill will “empower abusers,” by which we can only assume they are referring to women who engage in recreational sex. Lila Rose, an anti-abortion activist and president of Live Action, who has urged hundreds of thousands of social media followers to get off birth control, told the Washington Post “To be anti-fertility is to be anti-woman, and the proliferation of hormonal birth control is just another way of trying to force women to be more like men, with significant consequences for our emotional and physical health.”
The disinformation campaign is effective. The Washington Post article quotes as an example Catherine Miller, a 20-year-old junior at the University of Wisconsin at Stout. Miller reacted to the incoming stream of TikTok videos this way: “It created this sense of fear that if I ever needed to be put on birth control, I would become a completely different person, I would gain a bunch of weight, and my life would be over. I was like, well, obviously, this is true. This applies to everybody, because it’s the only thing I’m seeing.” Physicians report having to counteract an explosion of similar perceptions among young women bombarded on TikTok and Instagram.
Birth control pills do, like any other marketed pharmaceutical, have actually observed rare potential side-effects that must be listed on their packaging and which doctors are encouraged to discuss with prospective users. Among those warnings for so-called combination pills that contain both estrogen and progestin, are ones for blood clots and strokes. But the FDA points out that “the risk of developing blood clots from using birth-control pills — 3 to 9 women out of 10,000 who are on the pill — remains lower than the risk of developing blood clots in pregnancy and in the postpartum period. Doctors note that Opill… contains only progestin — meaning it does not have the blood clot risk of estrogen-containing pills.” IUDs have a low risk of perforating the uterine wall. But there are also lower-level risks (to be discussed in the next Section) that are often not adequately explained by physicians advising young women about the choice of contraceptives.
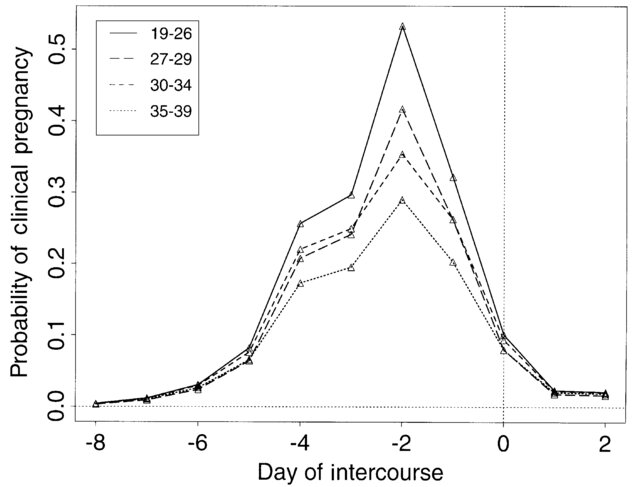
The anti-abortion and conservative activists behind the disinformation campaign are promoting, and sometimes even marketing, “natural family planning” alternatives to hormonal birth control. The most popular among these are smart phone apps that aid women in tracking the progress of their menstrual cycles, so they may avoid unprotected (i.e., condoms are acceptable) sex during the days preceding and just following ovulation. As shown by research in Fig. III.1, the probability of pregnancy following unprotected intercourse is at least a few percent for six days prior through two days after ovulation, given that sperm typically can survive for about five days in a woman’s reproductive system. Attempts to avoid sex during those eight days go back to the Rhythm Method of pregnancy avoidance introduced by a Catholic physician in the 1930s. Rhythm has no side-effects but has proven not very effective for pregnancy prevention.
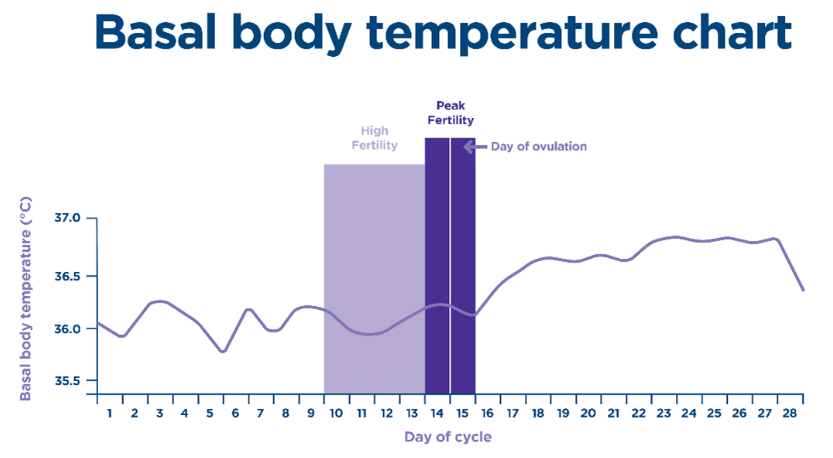
In her 1995 book Taking Charge of Your Fertility, Toni Weschler described how to take advantage of subtle body temperature changes to track the menstrual cycle more accurately than counting calendar days. As seen in Fig. III.2, the temperature changes are subtle and really occur only after ovulation, when temperature typically rises by 0.5—1.0°C. Women who rely on this method have to take their basal body temperature daily or nearly daily – i.e., “as soon as you wake up, before you even get out of bed. Take your temperature before you talk, eat, drink, have sex, check your phone — take your temperature before you do ANYTHING. Keep the thermometer in place for about five minutes.”
The first app approved by the FDA for contraceptive use in determining times of increased fertility is Natural Cycles. Millions of users pay $100 per year or $12.99 per month for a smart phone app that records and tracks their self-measured daily basal body temperature readings and indicates whether the day is green (infertile, OK for unprotected intercourse) or red (fertile) – see the display in Fig. III.3. As seen in Fig. III.2, that method is most reliable for telling you after your ovulation is completed; it cannot be very reliable for distinguishing fertile from infertile days prior to ovulation because any signal tends to be masked by ordinary day-to-day temperature fluctuations. So for advice prior to ovulation the app relies on learning the user’s menstrual cycle patterns, to the extent that those patterns are reproducible.

Other cycle-tracking apps use information in addition to basal body temperature: information about past periods, sleep patterns, heart rate, and the nature of cervical fluid issued in daily vaginal discharges. A 2019 analysis by Grand View Research found the market for women’s health apps growing by nearly 18% per year, with cycle-tracking apps dominating that growth. We will compare the efficacy for pregnancy protection of such app-supported cycle-tracking – what we refer to as the AlgoRhythm Method – to hormonal birth control options in Section IV.
Brittany Martinez, the founder of the conservative Evie magazine, has co-founded a competitor cycle-tracking app called 28, with financial backing from ultra-conservative tech mogul Peter Thiel. The app’s website states that “hormonal birth control promised freedom but tricked our bodies into dysfunction and pain.” But rather than recording body measurements, 28 appears primarily to offer fitness recommendations based on calendar determinations of where the user is within her own menstrual cycle.
Another form of marketing by TikTok anti-contraception activists is exemplified by Nicole Bendayan, who has started a “holistic-health coaching business” tracked by more than a million followers on TikTok and Instagram. Based on her own experience, “Bendayan has told her followers that birth control may deplete magnesium, vitamins B, C and E, and zinc levels. She charges hundreds of dollars for a three-month virtual program that includes analyses of blood panels for what she calls hormonal imbalances.” A recent Time Magazine analysis of such “hormone balancing” apps reports that they are built “from the rejiggered pieces of valid concepts…[but] There’s a clear disconnect between the guidelines and measurements clinicians use to diagnose endocrine disorders and the nonexistent metrics of ‘hormone balancing.’” Indeed, TikTok “specialists” tend to invoke hormone imbalance as an explanation for whatever ails a user, either physically or emotionally.
In summary, the birth control disinformation campaign is being driven by anti-abortion and right-wing activists, with a sprinkling of social media influencers seeking to make some money off confused young women. And their efforts are being funded by dark money groups associated with such conservative heavyweights as the Heritage Foundation, Charles Koch, Leonard Leo, and Peter Thiel.
IV. Hormonal contraceptives vs. fertility tracking
There are many different options available for contraception. The pie chart in Fig. IV.1 shows the usage rates of the different options from 2017 to 2019 by American women of childbearing age. In particular, there are a number of different types of hormonal birth control and a number of different natural family planning methods. The pie chart shows that some 40% of American women who rely on some form of contraception use hormonal contraceptives. In comparisons of the different options, three considerations come into play: efficacy in preventing pregnancy, ease of use, and side-effects.

Some of the hormonal options are semi-permanent, lasting for months to years, so they do not rely on a patient’s consistency of usage. For example, a small implantable rod placed under the skin of the upper arm releases enough of the hormone progestin daily to prevent pregnancy for up to three years, with measured efficacy above 99%. A T-shaped hormonal IUD can stay within the uterus for as long as five years, or until a woman wants it removed, and releases hormones that suppress ovulation with an efficacy again above 99%.
For most other methods, both hormonal and natural, efficacy is usually expressed under conditions of “perfect use” (e.g., take the pill at the same time every day) and “typical use,” allowing for the fact that most people are unable to always do things the exact same way every day and every month. For example, a birth control shot (Depo-Provera in Fig. IV.1, injection with a man-made hormone similar to the natural hormone progesterone) has an efficacy above 99% if injections are acquired no more than 13 weeks apart, but the efficacy falls to about 94% under typical use, when women wait longer between shots. The most common type of birth control pill, which combines doses of estrogen and progesterone to suppress ovulation, has a perfect use efficacy of 99% but a typical use efficacy (missing pills occasionally) of about 91%. The “minipill”, such as Opill, which uses progestin only has similar efficacy ratings, but perfect use is harder to attain as the pill must be taken at the same time (within 3 hours) every day, since progestin is cleared from the body more quickly than estrogen. Both kinds of birth control pill have multiple effects: suppressing ovulation, thickening cervical mucus to increase resistance to sperm, and thinning the lining of the uterus to hinder implantation. But the combination pill is more effective at the first of these than is the minipill.
The traditional rhythm method of natural family planning has an efficacy of only about 76%, less effective than relying on withdrawal or condoms to prevent pregnancy. What we have labeled algoRhythm – the use of mobile fertility-tracking apps to determine periods of high fertility during the menstrual cycle – is not, in general, much better than traditional reliance on the calendar and counting days. For example, one 2021 survey of married women in the country of Jordan found that of 119 participants who used such apps for contraceptive purposes, avoiding intercourse during days designated as fertile, 38 (or 31.9%) reported unintended pregnancies. Of those 38, half relied solely on the fertility-tracking apps for contraception.
The founders of the Natural Cycles app argue that they should not be lumped together with many other fertility-tracking apps. Elina Berglund, the co-founder and CEO of Natural Cycles has said: “As the first and only contraceptive app cleared by the FDA in the US and CE marked in Europe, our medical team has invested many resources into clinical studies that prove the effectiveness of our product. Other apps have not and while it hurts us as a company being lumped into a category of other apps that do not have the proper evidence, it also hurts women who may not understand the implications of downloading an app that will not work for her own personal needs.” Natural Cycles claims that its efficacy for preventing unintended pregnancy is 99% under perfect use and about 93% under typical use. These estimates are supported by five distinct surveys including data from as many as 70,000 women. It should be noted that all five surveys were financially supported by the company itself, and there have not yet been large independent surveys carried out.
The Natural Cycles app identifies the occurrence of ovulation by the consequent increases in both basal body temperature (BBT) and progesterone levels (see Fig. IV.2). But in predicting the fertility window the app relies on first learning the individual’s ovulation pattern during previous cycles, using that information to predict future ovulation days, and providing a safety margin by extending the fertility window on either side of the predicted ovulation day, by a number of days that depends on the user’s previous patterns. As seen in Fig. IV.2, that may leave only one or two days designated as “safe” between menstruation and ovulation. Hence, in practice, many users will be avoiding unprotected intercourse until after ovulation, when the physiological signals are much clearer. Such a delay would clearly help the efficacy results.

A perusal of customer ratings for Natural Cycles on Amazon and Trustpilot reveal a substantial number of complaints about accuracy in predicting ovulation, equipment malfunctions, subscription renewal practices, and the app sometimes changing days previously labeled green to red retroactively, which is not of much use to those who used the indication to have intercourse. Some other users who posted reviews of the app on the Google Play Store point out that the app is not for everyone because of the assumptions it makes about the quantity of sleep and the regularity of waking-up time. One user put it this way: “Honestly, this app is only useful if you are a very specific person with a very specific set of circumstances. As someone who is self-employed with irregular sleeping patterns and inconsistent schedule, the algorithm was pretty much incapable of doing anything with my information because of the fluctuations in my measurements…Great if you’re on normal cycles. Not particularly helpful post-birth and breastfeeding.”
Nonetheless, most users of the app seem satisfied and, on the basis of the data available so far, Natural Cycles seems to be a competitive alternative to birth control pills, in contrast to nearly all other cycle-tracking apps. It has the important advantage of no medical side-effects, but in comparison with hormonal contraception it has the disadvantage of requiring users to adopt other contraceptive methods if they want to avoid abstinence during significant portions of each menstrual cycle.
What is known about the real side-effects of hormonal contraception, as opposed to many of the lies spread on social media? The American College of Obstetricians and Gynecologists (ACOG) lists the common side-effects as nausea, headaches, breast tenderness, and bleeding between periods. Some rare side-effects can lead women who have susceptibility to one or more of these risks to choose different types of hormonal birth control. For example, combination pills delivering doses of both estrogen and progestin are not recommended for women who have a history of blood clots, heart disease, migraine headaches, diabetes, liver disease, or heavy smoking. The progestin-only minipills, such as Opill, are safer for women with these susceptibilities, but not for women with some forms of lupus.
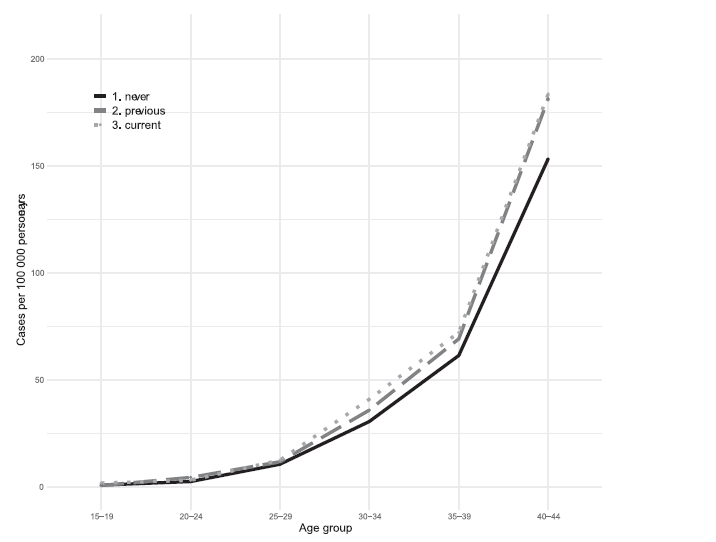
Both types of birth control pill appear to increase the risk of breast cancer very slightly. For example, a survey of 1.5 million Swedish women found the results shown in Figs. IV.3-4, which suggest a possible increase in probability of breast cancer by 0.03% among current users of either combination or progestin-only pills.

And what of reports from some hormonal contraceptive users (and numerous disinformation spreaders) that these methods diminish a woman’s libido, which is certainly a possible reaction given that the contraceptives tend to lower circulating testosterone levels? A systematic review of 36 independent studies carried out between 1978 and 2011 found that among a total of 8,422 women taking the combination birth control pill 22% reported an increase in their libido, 15% reported a decrease, and 64% reported no change. It seems, as with most pharmaceuticals, that birth control pills affect different women in different ways.
In 2016 tech journalist Kate Bevan encouraged combination pill users to share their stories on social media using the hashtag #MyPillStory. Posts with such hashtags are overwhelmingly dominated by users reporting adverse experiences, including nausea, depression, and anxiety. For counterbalance, most surveys find the clear majority of women on birth control pills to be satisfied with the contraceptive’s operation and effect on them. For example, one survey of 1303 West German women taking oral contraceptives found 68% to be satisfied, with negative mood changes reported by only 16%. However, on both social media and other surveys, a common complaint is that doctors never warned the women sufficiently about the side-effects or about possible interactions with other drugs.
The #MyPillStory posts are fine and indeed represent one of the benefits of social media in fostering far-flung support groups. These posts have contributed in part to a decrease in pill users in recent years, accompanied by an increase in IUD users as well as those who use cycle-tracking apps. But the weight given to those one-sided personal stories by young women today usually far exceeds that given to opinions or epidemiological research by health professionals. The real problem occurs when those negative stories have been picked up, amplified, and mixed with lies and half-truths by anti-abortion activists behind the current disinformation surge.
Also lost in the social media whirlwind are stories of other benefits, besides contraception, offered by birth control pills. Clinical studies have demonstrated that consistent use of the combination birth control pill brings about significant reductions in the following common female medical conditions: severe menstrual cramps (dysmenorrhea); heavy menstrual bleeding (menorrhagia); endometriosis (migration of uterine lining tissue outside the uterus); acne and hirsutism caused by polycystic ovary syndrome (PCOS); long-term risk of developing cancer of the ovary and the endometrium. Occasionally reported benefits for bone health, colon cancer, and benign breast disease are less well established clinically. Although there is no evidence that oral contraceptives suppress cervical infections, there is also no evidence that they cause any significant increase in risk for sexually transmitted infections, despite some claims to the contrary among the ongoing disinformation campaign.
V. hidden agendas
There is no problem with women sharing their negative experiences with birth control pills on social media, via the #MyPillStory hashtag. This is one source of information for young women deciding their reproductive futures – one-sided information, but information nonetheless. It would be good if those posts lead physicians to do a better job informing women about their choice of options for contraception and the advantages and potential drawbacks of each option, as well as working with them to change options when a woman experiences negative impacts from her previous choice. As we have seen above, no option is right for everyone; there are complaints about every option. But the important point is to maintain the range of options.
The problem arises when the negative experiences women have shared get amplified and embellished with lies in a disinformation campaign whose goal is to narrow the range of choices available to women. This campaign is being driven by anti-abortion activists and Christian Nationalists, whose avowed aim is to impose bans on all forms of “non-natural” contraception. Here, we try to analyze what is really driving this anti-contraception stance.
Pregnancy can first be detected by emission of the hormone hCG (human chorionic gonadotrophin), which signals successful implantation of an embryo in a woman’s uterine lining. Implantation, if it occurs, usually takes place 10-11 days after fertilization of an egg to form a single-celled zygote. But zygote formation cannot be detected inside a woman’s body. Progesterone levels normally increase after ovulation, as seen in Fig. IV.2, and may be even higher if conception occurs, but cannot reliably pinpoint zygote formation. Hence, the U.S. federal definition of pregnancy as beginning at implantation is a sensible one – it relies on measurable hormonal changes. Abortion, by legal definition, is a medical intervention to terminate a pregnancy. Abortion cannot logically occur before a pregnancy has begun.
Contraception is aimed at preventing pregnancy and is thus clearly distinguishable from abortion. Most hormonal contraceptives operate primarily by suppressing ovulation and increasing resistance to the flight of sperm toward an egg. Occasionally, when these methods fail, hormonal contraceptives may also prevent pregnancy by impeding implantation. All of these methods take effect prior to the beginning of pregnancy, so they cannot be confused with abortion. Furthermore, there is a large body of evidence outlined in Section II that modern contraceptives are efficient in reducing the incidence of abortions by reducing unintended pregnancies.
So why do anti-abortion activists want to ban contraception as well? Their stated justification is that they want to protect all human life, which in their view begins at the formation of a zygote; anything that hinders the development and implantation of the resulting embryo should be considered an abortion. But this “personhood” justification doesn’t make much logical sense for a legal standard. For one thing, it attempts to tie a legal phenomenon – the beginning of a new life – to an event that is not clearly detectable (except in in vitro fertilization, IVF, where the zygote is formed outside the woman’s body). For a second thing, personhood would probably lead, as seen in the recent Alabama Supreme Court decision, to declaring IVF procedures illegal, when IVF is a broadly supported method for generating more human lives.
For a third reason, personhood would imply that human biology is responsible, without intervention, for the death of a substantial portion of initiated life (the same is true for all mammals). As best we can determine from data to date, even under normal conditions as many as 40% of eggs fertilized in vivo fail to make it to successful implantation (see Fig. V.1). The natural roadblocks along that ten-day path involve: chromosomal abnormalities that may develop either during fertilization or during the many subsequent cell divisions needed to develop the embryo; possible unsuccessful transit through the fallopian tubes to the uterus, sometimes terminating in non-viable ectopic pregnancies that pose strong danger to a woman’s life; possible unsuccessful implantation in the uterine lining. Declaring that new life begins at fertilization is akin to declaring that the start of a new major space telescope like the James Webb (or pick your own favorite large project) is at the time of the first sketch on a napkin. There are many hurdles to pass to get to a successful launch, just as there are many hurdles for a zygote to pass before it can launch a pregnancy.

We don’t believe that all of the Christian Nationalists pushing an anti-contraceptive agenda are ignorant of the above science, or even believe that their religion actually “determines” the starting point for new life. In fact, traditional religions have little to say on the subject because when these religions were launched there was little understanding of the processes of birth. The Catholic Church did not adopt the view that a human soul is developed at conception until 1869, when Pope Pius IX decided that view was necessary for theological consistency with the view of the Immaculate Conception of Jesus. Other religions, such as Judaism, believe new life to begin at birth. The point is that the starting point of a new life is a philosophical debate, while the starting point of a pregnancy can be tied to detectable hormonal changes.
Instead, we believe leading Christian Nationalists have hidden agendas. Few of the proponents of “Making American Great Again” are ever asked when they think America was last great. If pushed, we suspect that most would put the “great” period before what Nobel Prize-winning economist Claudia Goldin has dubbed the “Quiet Revolution” of the second half of the 20th century. The Quiet Revolution refers to the rapid and voluminous entry of American women into the workforce, into higher education, and even into government after they attained control over their own reproductive choices. A seminal event in attaining that control was the FDA approval of the first birth control pill for contraceptive use in 1960. A secondary spur was the 1973 Supreme Court ruling in Roe v. Wade granting a constitutionally protected right to abortion.
Of course, some Christian Nationalists would prefer to go back much further than 1950; current Republican Speaker of the U.S. House of Representatives told an anti-abortion gathering that we need to get back to “18th-century values.” The 18th century is convenient because it was before women received much education, well before they could vote, and women’s place was clearly understood to be in maintaining the home and raising babies. Many right-wing conservatives believe that the alteration of such “traditional” gender roles has weakened families and the nation’s moral fiber, and that contraceptives bear much of the blame.
But there is more at stake than just wishing to return women to centuries-old roles. As we pointed out in detail in our previous post on The Accelerating Worldwide Baby Bust, that Quiet Revolution, now spread throughout the developed world, has led to rapid declines in fertility around the world. In most developed countries today, the average fertility rates have fallen well below the level (2.1 live births per woman) needed to maintain constant population. The implication of this fertility decline is that global human population will peak later during this century, and that in developed countries a dwindling workforce will have to provide income, revenue, and services to support a growing senior population.
The map in Fig. V.2 indicates the projected changes by 2050 in the number of working age people in many countries. Low fertility rates are represented by losses denoted by orange circles. The vast majority of gains, denoted by green circles, are in countries which still have high (though declining) fertility rates. But the U.S., Canada, and Australia all have fertility rates below replacement level and get small projected increases in working age population nonetheless, due to their welcoming immigration policies. Worldwide, immigration is seen as the most effective way in the 21st century to counteract dwindling working-age and growing senior populations that accompany declining fertility rates and improvements in life expectancy.

But right-wing conservatives and most Republican legislators oppose liberal immigration policies because they fear the loss of power to people of different backgrounds, ethnicities, and races. How does one oppose immigration but still try to address the economic and social problems that will accompany a dwindling and aging population? By banning hormonal contraceptives and favoring instead “natural family planning” or “algoRhythm,” which has traditionally led to a much higher rate of unintended pregnancies than hormonal contraceptives. For the anti-contraceptive crowd, the frequent failures of most fertility awareness methods are not a bug, but a desirable feature to increase fertility.
The problem the contraceptive opponents face is that worldwide evidence suggests that a growth in unintended pregnancies will be accompanied by a substantial increase in abortions (even in countries with very restrictive abortion laws), giving the lie to their expressed concern for the life of the unborn. So instead of admitting to their hidden agendas, they choose to violate common sense by conflating contraception with abortion, and simultaneously to engage in a disinformation campaign aimed at frightening young women off the use of hormonal contraceptives. If you can’t convince women to surrender their rights to reproductive choice, convince the most impressionable among them instead that most of their options will do them great harm.
References:
Q. Forgey and J. Gerstein, Justice Thomas: SCOTUS ‘Should Reconsider’ Contraception, Same-Sex Marriage Rulings, Politico, June 24, 2022, https://www.politico.com/news/2022/06/24/thomas-constitutional-rights-00042256
Griswold v. Connecticut, https://www.oyez.org/cases/1964/496
Eisenstadt v. Baird, https://supreme.justia.com/cases/federal/us/405/438/
Wikipedia, Federalist Society, https://en.wikipedia.org/wiki/Federalist_Society
Wikipedia, Leonard Leo, https://en.wikipedia.org/wiki/Leonard_Leo
H.H. Manning, The Conservative Position on Birth Control is About Individual Responsibility, New York Times, June 24, 2023, https://www.nytimes.com/2023/06/24/opinion/pro-life-birth-control-abortion.html
Ballotpedia, History of Abortion Ballot Measures, https://ballotpedia.org/History_of_abortion_ballot_measures
A.B. Wang and L.A. Caldwell, 12 States Where the Fate of Abortion Rights Could Be on 2024 Ballots, Washington Post, Dec. 20, 2023, https://www.washingtonpost.com/politics/2023/12/20/abortion-rights-2024-ballot-measures/
N. El-Bawab, Here’s Where Abortion is Banned 3 Months After Roe v. Wade Was Overturned, ABC News, Sept. 24, 2022, https://abcnews.go.com/US/abortion-banned-months-roe-wade-overturned/story?id=90262760
PRRI, The State of Abortion and Contraception Attitudes in All 50 States, https://www.prri.org/research/legal-in-most-cases-the-impact-of-the-abortion-debate-in-2019-america/
Wikipedia, Humanae Vitae, https://en.wikipedia.org/wiki/Humanae_vitae
R.K. Jones and J. Dreweke, Countering Conventional Wisdom: New Evidence on Religion and Contraceptive Use, Guttmacher Institute, April 2011, https://www.guttmacher.org/sites/default/files/pdfs/pubs/Religion-and-Contraceptive-Use.pdf
L. Weber and S. Malhi, Women Are Getting Off Birth Control Amid Misinformation Explosion, Washington Post, March 21, 2024, https://www.washingtonpost.com/health/2024/03/21/stopping-birth-control-misinformation/
Mayo Clinic, Rhythm Method for Natural Family Planning, https://www.mayoclinic.org/tests-procedures/rhythm-method/about/pac-20390918
J. Dreweke, Contraception is Not Abortion: The Strategic Campaign of Anti-abortion Groups to Persuade the Public Otherwise, Guttmacher Policy Review, Fall 2014, https://www.guttmacher.org/sites/default/files/article_files/gpr170414.pdf
A. Demirhan, Anti-Abortion Groups are Coming for Birth Control – Just as Reproductive Rights Activists Warned, Ms. Magazine, Aug. 17, 2023, https://msmagazine.com/2023/08/17/anti-abortion-pro-life-over-the-counter-birth-control-women/
K. Butler, Inside Anti-Abortion Groups’ Campaign to Sell Women on Unreliable Birth Control “Alternatives”, Mother Jones, Sept. 30, 2022, https://www.motherjones.com/politics/2022/09/inside-anti-abortion-groups-campaign-to-sell-women-on-unreliable-birth-control-alternatives/
J. Amy, EXPLAINER: What’s the Role of Personhood in Abortion Debate?, AP News, July 30, 2022, https://apnews.com/article/abortion-us-supreme-court-health-government-and-politics-constitutions-93c27f3132ecc78e913120fe4d6c0977
Cornell Law School, 45 CFR § 46.202 – Definitions, https://www.law.cornell.edu/cfr/text/45/46.202
G.E. Jarvis, Estimating Limits for Natural Human Embryo Mortality, F1000 Research 5, 2083 (2016), https://f1000research.com/articles/5-2083/v2
J. Sharfstein, The Alabama Supreme Court’s Ruling on Frozen Embryos, Bloomberg School of Public Health, Feb. 27, 2024, https://publichealth.jhu.edu/2024/the-alabama-supreme-courts-ruling-on-frozen-embryos
Alabama Senator Offers Confusing Response to IVF Question, https://www.youtube.com/watch?v=ayBo9kXAIvQ
G. Sparks, et al., KFF Health Tracking Poll: Early 2023 Update on Public Awareness on Abortion and Emergency Contraception, KFF, Feb. 1, 2023, https://www.kff.org/womens-health-policy/poll-finding/kff-health-tracking-poll-early-2023/
U.S. Food and Drug Administration, Plan B One-Step (1.5 mg Levonorgestrel) Information, https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/plan-b-one-step-15-mg-levonorgestrel-information
Collaborative for Reproductive Equity, A Surprising Number of Physicians Believe Some Contraceptives Work by Causing Abortion, Nov. 9, 2022, https://core.wisc.edu/2022/11/09/core-study-finds-a-surprising-number-of-physicians-believe-contraceptives-cause-abortion/
J. Bearak, et al., Unintended Pregnancy and Abortion by Income, Region, and the Legal Status of Abortion: Estimates from a Comprehensive Model for 1990-2019, Lancet Global Health 8, e1152 (2020), https://www.thelancet.com/action/showPdf?pii=S2214-109X%2820%2930315-6
D.D. Williams, Access to Free Birth Control Reduces Abortion Rates, Washington University School of Medicine, Oct. 12, 2012, https://medicine.wustl.edu/news/access-to-free-birth-control-reduces-abortion-rates/
J. Bearak, et al., Global, Regional, and Subregional Trends in Unintended Pregnancy and its Outcomes from 1990 to 2014: Estimates from a Bayesian Hierarchical Model, Guttmacher Institute, March 2018, https://www.guttmacher.org/article/2018/03/unintended-pregnancy-and-its-outcomes-global-regional-and-subregional-trends-1990
J. LeMieux, Dear America, Contraception Works, American Council on Science and Health, May 4, 2017, https://www.acsh.org/news/2017/05/04/dear-america-contraception-works-11220
A. Deschner and S.A. Cohen, Contraceptive Use is Key to Reducing Abortion Worldwide, Guttmacher Institute, Oct. 1, 2003, https://www.guttmacher.org/gpr/2003/10/contraceptive-use-key-reducing-abortion-worldwide
J. Bongaarts and D. Hodgson, The Impact of Voluntary Family Planning Programs on Contraceptive Use, Fertility, and Population, in Fertility Transition in the Developing World, Sept. 2022, https://www.researchgate.net/publication/363184369_The_Impact_of_Voluntary_Family_Planning_Programs_on_Contraceptive_Use_Fertility_and_Population
Wikipedia, One-Child Policy, https://en.wikipedia.org/wiki/One-child_policy
C. Marston and J. Cleland, Relationships Between Contraception and Abortion: a Review of the Evidence, International Family Planning Perspectives 29, 6 (2003), https://pubmed.ncbi.nlm.nih.gov/12709307/
G.M. Secura, et al., Provision of No-Cost, Long-Acting Contraception and Teenage Pregnancy, New England Journal of Medicine 372, 297 (2015), https://www.nejm.org/doi/10.1056/NEJMx140061
Guttmacher Institute, The Percentage of Unintended Pregnancies Ending in Abortion Has Increased in Countries Where Abortion is Restricted, https://www.guttmacher.org/infographic/2020/percentage-unintended-pregnancies-ending-abortion-has-increased-countries-where
Right to Contraception Act, 117th Congress, https://www.congress.gov/bill/117th-congress/house-bill/8373?r=2&s=1
DebunkingDenial, Brainwashing via Social Media, https://debunkingdenial.com/brainwashing-via-social-media/
M. Wenner, Birth Control Pills Affect Women’s Taste in Men, Scientific American, Dec. 1, 2008, https://www.scientificamerican.com/article/birth-control-pills-affect-womens-taste/
DebunkingDenial, Wellness Fads, https://debunkingdenial.com/portfolio/wellness-fads/
Live Action, https://www.liveaction.org/
D.B. Dunson, B. Colombo, and D.D. Baird, Changes with Age in the Level and Duration of Fertility in the Menstrual Cycle, Human Reproduction 17, 1399 (2002), https://www.researchgate.net/publication/11388268_Changes_with_age_in_the_level_and_duration_of_fertility_in_the_menstrual_cycle
T. Weschler, Taking Charge of Your Fertility, https://www.tcoyf.com/taking-charge-of-your-fertility/
Planned Parenthood, What’s the Temperature Method of FAMs?, https://www.plannedparenthood.org/learn/birth-control/fertility-awareness/whats-temperature-method-fams
Clearblue, Basal Body Temperature: What Is It, How to Chart It, and More, https://www.clearblue.com/how-to-get-pregnant/basal-body-temperature
Natural Cycles, https://www.naturalcycles.com/
J. Bull, et al., Typical Use Effectiveness of Natural Cycles: Postmarket Surveillance Study Investigating the Impact of Previous Contraceptive Choice on the Risk of Unintended Pregnancy, BMJ Open 9, e026474 (2019), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6475236/pdf/bmjopen-2018-026474.pdf
K.M. Robinson, Wellness Apps You Can Use to Track Birth Control, WebMD, https://www.webmd.com/sex/birth-control/features/birth-control-apps
28 Wellness App, https://28.co/
H. Weiss, You Don’t Need to Balance Your Hormones, Time Magazine, May 9, 2023, https://time.com/6277941/balance-hormones-cycle-syncing-myth/
R. Lehmann-Haupt, The Future of Birth Control, https://proto.life/2022/05/the-future-of-birth-control/
WebMD, Nexplanon Implant – Uses, Side Effects, and More, https://www.webmd.com/drugs/2/drug-156597/nexplanon-subdermal/details
P. Frysh, How Effective are Different Types of Birth Control?, WebMD, July 13, 2023, https://www.webmd.com/sex/birth-control/birth-control-effectiveness-chart
WebMD, Depo-Provera (Birth Control Shot), https://www.webmd.com/sex/birth-control/birth-control-depo-provera
F. Al-Rshoud, et al., The Use and Efficacy of Mobile Fertility-Tracking Applications as a Method of Contraception: A Survey, Current Obstetrics and Gynecology Reports 10, 25 (2021), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8009922/
K. Hunt, Fertility Apps Can Be ‘Misleading’ for Women, Review Finds, CNN, April 7, 2020, https://www.cnn.com/2020/04/06/health/fertility-period-contraceptive-apps-trackers-wellness/index.html
National Institute for Health and Care Excellence, Natural Cycles for Monitoring Fertility, Jan. 19, 2021, https://www.nice.org.uk/advice/mib244/resources/natural-cycles-for-monitoring-fertility-pdf-2285965632946885
Amazon.com, Customer Reviews for Natural Cycles App, https://www.amazon.com/Natural-Cycles-Month-Subscription-Thermometer/product-reviews/B08B8XT4BM
Trustpilot.com, Customer Reviews for Natural Cycles App, https://www.trustpilot.com/review/www.naturalcycles.com
M.C. Felice, M.L.J. Søndergaard, and M. Balaam, Analyzing User Reviews of the First Digital Contraceptive: Mixed Methods Study, Journal of Medical Internet Research 25, e47131 (2023), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10685276/
Planned Parenthood, How Safe is the Birth Control Pill?, https://www.plannedparenthood.org/learn/birth-control/birth-control-pill/how-safe-is-the-birth-control-pill
J.L. Hultstrand, et al., Hormonal Contraception and Risk of Breast Cancer and Breast Cancer in Situ Among Swedish Women 15-34 Years of Age: A Nationwide Register-Based Study, The Lancet Regional Health 21, 100470 (2022), https://www.thelancet.com/journals/lanepe/article/PIIS2666-7762(22)00166-1/fulltext
Z. Pastor, K. Holla, and R. Schmel, The Influence of Combined Oral Contraceptives on Female Sexual Desire: a Systematic Review, European Journal of Contraceptive and Reproductive Health Care 18, 27 (2013), https://pubmed.ncbi.nlm.nih.gov/23320933/
M. Friedman, Women Are Sharing Their Terrifying Birth Control Stories Online, Cosmopolitan, Apr. 4, 2016, https://www.cosmopolitan.com/health-fitness/news/a56237/mypillstory-side-effects-birth-control-pill/
B.J. Oddens, Women’s Satisfaction with Birth Control: A Population Survey of Physical and Psychological Effects of Oral Contraceptives, Intrauterine Devices, Condoms, Natural Family Planning, and Sterilization Among 1466 Women, Contraception 59, 277 (1999), https://www.sciencedirect.com/science/article/abs/pii/S0010782499000347
A. Schneider-Kamp and J. Takhar, Interrogating the Pill: Rising Distrust and the Reshaping of Health Risk Perceptions in the Social Media Age, Social Science and Medicine 331, 116081 (2023), https://www.sciencedirect.com/science/article/pii/S0277953623004380?via%3Dihub
D.T. Baird, et al., Noncontraceptive Health Benefits of Combined Oral Contraception, Human Reproduction Update 11, 513 (2005), https://www.researchgate.net/publication/299057805_Noncontraceptive_health_benefits_of_combined_oral_contraception
K. Rissman, Republicans Are Taking Aim on Contraception – and They’d Rather You Didn’t Know, The Independent, Feb. 12, 2024, https://www.the-independent.com/news/world/americas/us-politics/republicans-contraception-abortion-2024-election-b2493130.html
D.D. Baird, et al., Preimplantation Hormonal Differences Between the Conception and Non-conception Menstrual Cycles of 32 Normal Women, Human Reproduction 12, 2607 (1997), https://pubmed.ncbi.nlm.nih.gov/9455822/
S. Simmons-Duffin, L.A. Johnson, and M. Rizzo, The Surprising Science of How Pregnancy Begins, NPR, Apr. 12, 2023, https://www.npr.org/sections/health-shots/2023/04/12/1159753316/pregnancy-start-conception
Mayo Clinic, Ectopic Pregnancy, https://www.mayoclinic.org/diseases-conditions/ectopic-pregnancy/symptoms-causes/syc-20372088
P. McGarry, Catholic Church Teaching on Abortion Dates from 1869, Irish Times, July 1, 2013, https://www.irishtimes.com/news/social-affairs/religion-and-beliefs/catholic-church-teaching-on-abortion-dates-from-1869-1.1449517
G.E. Jarvis, Misjudging Early Embryo Mortality in Natural Human Reproduction, F1000 Research 9, 702 (2020), https://f1000research.com/articles/9-702/v1
H. Leridon, Intrauterine Mortality, in H. Leridon, Human Fertility: The Basic Components (University of Chicago Press, 1977), https://www.ncbi.nlm.nih.gov/nlmcatalog/100987173
C. Goldin, The Quiet Revolution That Transformed Women’s Employment, Education, and Family, Richard T. Ely Lecture, 2006, https://pubs.aeaweb.org/doi/pdfplus/10.1257/000282806777212350
S.W. Junod, FDA’s Approval of the First Oral Contraceptive, Enovid, U.S. Food and Drug Administration, https://www.fda.gov/media/110456/download
K. Pollitt, Mike Johnson’s “18th-Century Values”, The Nation, Nov. 30, 2023, https://www.thenation.com/article/society/mike-johnson-values/
DebunkingDenial, Ramifications of the Accelerating Worldwide Baby Bust, https://debunkingdenial.com/ramifications-of-the-accelerating-worldwide-baby-bust-part-i-data-and-causes/
A. Taub and L. Leatherby, How Shrinking Populations Fuel Divisive Politics, New York Times, Feb. 2, 2024, https://www.nytimes.com/2024/02/02/world/europe/interpreter-shrinking-populations-fuel-divisive-politics.html
