
June 19, 2025
I: Introduction
The COVID-19 pandemic was deadly: it led to more than 7 million human deaths worldwide and more than one million in the U.S. alone, mutating along the path into several different strains that caused a number of infection surges. And yet it could have been worse. By the end of 2020 vaccines had been developed and subjected to clinical tests to help prevent both the spread and the most serious impacts of the virus. After the vaccines became widely available within the U.S. the death rate among individuals who remained unvaccinated was an order of magnitude higher than that among people who received two vaccinations, as shown in Fig. I.1.

Figure I.1. Comparison of COVID-19 death rates (deaths per 100,000 people) in the U.S. after Fall 2021 between unvaccinated individuals (red curve) and those vaccinated without (green) or with (blue) the bivalent booster shot that became available in 2022. The plot is from Our World in Data.
The COVID vaccines were developed in world-record time. Before COVID the shortest time taken to process a vaccine from development to deployment was the four-year development time for the mumps vaccine in the 1960s. In an important medical breakthrough, the development of the COVID vaccines was compressed to only one year, thanks in part to funding from the Operation Warp Speed program initiated by the first Trump administration and in part to competition among a number of research groups worldwide. The mechanism used by the Pfizer and Moderna vaccines was novel, although it had been in development for other purposes for decades. They both used synthesized messenger RNA (mRNA) to get targeted cells to produce proteins simulating the spike proteins that surround a SARS-CoV-2 virus, in order to train the immune system to recognize and neutralize the virus before it caused severe infection. One benefit of the mRNA approach is that it could be straightforwardly updated to handle the new strains of the virus that evolved during the pandemic.
Because the vaccines were novel and the operation of mRNA in human cells was not widely understood, even apparently by some physicians, the community of people who opposed vaccines in general was able to spread a considerable amount of misinformation and conspiracy theories about the Pfizer and Moderna vaccines. That misinformation has morphed by now into a full-blown demonization campaign against mRNA vaccines. One of the prominent deniers of mRNA technology is Robert F. Kennedy, Jr., the current Secretary of Health and Human Services (HHS). Following his leadership, a number of states with Republican leadership are now debating bills that would ban or severely limit the use of mRNA technology in vaccines. Furthermore, HHS has recently terminated funding for Moderna to develop an mRNA vaccine against bird flu, which threatens to fuel the next pandemic. It is important that some actual scientific information be injected into the ongoing conversations about mRNA vaccines.
II. Some Basics of Cell Biology
In order to appreciate how mRNA vaccines work, one needs to understand a few basics of cell biology. Humans share a basic cell structure with all other animals (see Fig. II.1), characterized by a nucleus surrounded by a membrane, within which the DNA resides. The technical term for cells with bounded nuclei is eukaryotic. The cellular material outside the nucleus is called the cytoplasm. One of the cell’s central functions is to produce proteins. The instructions for protein assembly are contained within the genes inside the nucleus, but the actual assembly of proteins occurs in the cytoplasm at the sites marked ribosome in Fig. II.1. Messenger RNA, as the name suggests, is the biomolecule that carries the protein-building instructions from inside the nucleus to the cytoplasm. The mitochondria depicted in Fig. II.1 are the cell’s engines: using their own DNA inherited from the mother, they convert nutrients to chemical energy to power the cell’s biochemical reactions.
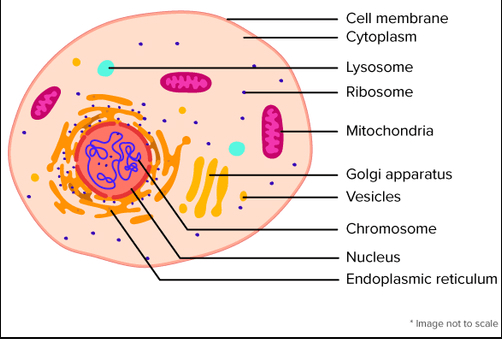
Figure II.2 illustrates the basic processes of transcription and translation by which cells synthesize proteins. A single-stranded mRNA molecule copies the relevant genes from one strand of the DNA inside the nucleus. The mRNA then migrates across the nuclear boundary into the cytoplasm. There it provides the instructions to assemble amino acids into a protein at one of the ribosome sites in the cytoplasm. Each amino acid is encoded by a three-base sequence within the gene copy carried by the mRNA. The C, A, G, and U labels on the mRNA molecule in Fig. II.2 refer to the four nitrogenous bases of RNA: cytosine, adenine, guanine, and uracil (replacing the thymine in DNA), respectively. Twenty-one distinct amino acids correspond to different three-letter sequences of C, A, G, and U.
Figure II.2. Schematic illustration of the processes of transcription and translation by which mRNA copies genes inside the cell’s nucleus, then migrates to a ribosome in the cytoplasm to provide the gene’s detailed instructions for assembling amino acids into proteins.
The basic structure of a SARS-CoV-2 virus cell is illustrated in Fig. II.3. The genetic material in many highly infectious viruses is contained in RNA, rather than DNA. One feature of the difference is that RNA replication is much more error-prone than DNA replication, explaining why viruses such as SARS-CoV-2 can mutate and evolve relatively quickly as they replicate themselves within a host cell. Virus cells are surrounded by surface proteins which aid their entry into host cells, as illustrated in Fig. II.4. Once inside a host cell, the virus releases its RNA and uses the cell’s own mechanisms to replicate itself and to produce viral proteins, as illustrated in Fig. II.5. Mutations during the viral RNA replication lead to evolved forms of the virus, some of which may be more virulent.
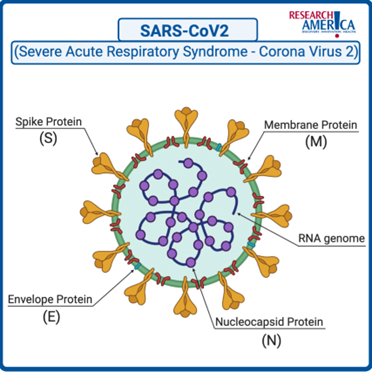
Figure II.3. The structure of the SARS-CoV-2 virus cell with surface spike proteins attached to the membrane surrounding the viral RNA.

Figure II.4. Viruses use their surface proteins to attach to receptors on the membrane of a host cell, enabling the virus to enter the cell.

Figure II.5. Illustration of the stages of viral infection. Once inside a host cell, the virus releases its RNA and uses the cell’s own mechanisms to replicate itself and to produce viral proteins.
The purpose of the body’s immune system is to recognize and kill dangerous intruder cells, generically called antigens. The role of vaccines is to train the immune system to recognize specific dangerous viruses, bacteria, and fungi by their surface proteins and to develop antibodies to disarm those invaders. Antibodies are specific proteins attached to the surface of particular white blood cells known as B lymphocytes. The body can produce an enormous variety of antibodies by random selection of gene segments within each lymphocyte cell. When the surface proteins of an invading virus, for example, bind to the antibodies on B lymphocyte cells, the antigens themselves become tagged for later recognition and destruction by other white blood cells. In addition, they trigger rapid multiplication of the lymphocyte cells into daughter clones, each of which expresses the same antibody, except for possible random mutations. Mutations to the antibodies that increase their binding attraction for the targeted antigens are naturally selected to improve the efficiency of the immune system fight against the related disease.
Traditional types of vaccine trained the immune system by injecting germ cells that have either been rendered inactive (i.e., unable to replicate themselves) or have been weakened. In either case, the germ cell’s surface proteins, by which they are to be recognized by B lymphocyte cells, are left intact. In contrast, mRNA vaccines do not inject viral RNA into the body at all. Rather they enter the cytoplasm of targeted cells, where the synthesized mRNA molecules contain the instructions to generate proteins that simulate the surface proteins of the germ cell. The immune system recognizes these new proteins as foreign and then generates antibodies to fight those same proteins when they enter the body on the surface of invading pathogen cells. The mRNA injected in the vaccine never enters cell nuclei, where they could potentially interact with the body’s own DNA.
With that background we can now address in subsequent sections the decades-long development of mRNA vaccines, their use in preventing COVID infections and potential uses for other diseases, and the organized demonization campaign that is threatening their continued development.
III: The Development of mRNA Vaccines
The development of mRNA vaccines occurred over a significant time period and involved the work of hundreds of researchers. In early days, there was little interest in mRNA for medical purposes, because there was no known mechanism for integrating messenger RNA into cells. But in 1987 graduate student Robert Malone, working at the Salk Institute for Biological Studies, experimented with mixing strands of mRNA with droplets of fat. He found that human cells immersed in the mRNA-fat mixture absorbed the mRNA and produced proteins from it. Malone himself was using techniques that had been discovered a decade earlier, where scientists used liposomes to transport mRNA into mouse and human cells in order to induce expression of proteins. But at the time, mRNA appeared to be so unstable that no medical products could be obtained from using it.
In 1989, after a dispute with his research advisor at the Salk Institute, Robert Malone left Salk without completing his doctoral degree. After that, the Salk Institute abandoned any patent claims for medical uses of mRNA. Various researchers attempted to use mRNA techniques to produce vaccines, but it seemed that these methods were too difficult. mRNA was notoriously prone to degradation, and it appeared that production of mRNA for vaccines would require enormous startup costs. Most research groups abandoned efforts to produce vaccines using mRNA, and instead focused on development of DNA vaccines. Although the production of DNA vaccines has proved slow and difficult, a number of the techniques developed for DNA vaccines proved to be useful in the creation of mRNA vaccines.
Over the next couple of decades, research on possible mRNA and DNA vaccines was taken up by a number of groups. It seemed that every group that made an advance in this field immediately founded companies and set out in search of venture capital. But there were two notable advances that eventually made possible the mRNA vaccines used to combat COVID-19. The first was a discovery by Katolin Karikó and Drew Weissman, shown in Fig. III.1, at the University of Pennsylvania. During trials with mice, Karikó and Weissman found that injection of their mRNA produced massive inflammatory reactions. However, they discovered that if the nucleotide uridine — a combination of uracil and ribose sugar, the molecule that makes up the backbone of RNA and DNA — in their mRNA molecule was replaced with pseudouridine, the mice no longer produced the inflammatory reaction. (Pseudouridine substitutes in a different bond between uracil and ribose than the one in uridine.) Apparently, the modification that used pseudouridine allowed the molecules containing mRNA to avoid the cells’ immune defenses.

Figure III.1: Katolin Karikó and Drew Weissman. They shared the 2023 Nobel Prize in Physiology or Medicine for the development of methods that allowed mRNA molecules to be delivered to the body to produce vaccines.
A second advance was made by biochemist Pieter Cullis of the University of British Columbia. Cullis created lipid nanoparticles or LNPs for delivering mRNA into the cells of the body. Eventually Cullis developed combinations of four fatty molecules, which surround the mRNA and carry it into the cells. The first three of these molecules provide structure and stability, while the fourth lipid is ionizable. Initially, this fourth lipid is positively charged; this enhanced the ability of the fatty molecule to link with the negatively charged mRNA backbone. However, Cullis also showed that when the LNPs entered the bloodstream, the positive charge turned off. This greatly decreased toxic effects of these LNPs on the body.
In the mid-2000s, various research groups all contributed to the development of vaccines that used mRNA techniques. Several companies were formed to utilize the modified mRNA due to Karikó and Weissman, and the lipid molecule structures developed by Cullis. These companies competed to produce mRNA vaccines. The two companies that eventually won out in the competition to produce a vaccine that would protect against the SARS-CoV-2 virus were Moderna and Pfizer/BioNTech. Their work culminated in the development of vaccines against COVID-19 in 2020. Figure III.2 shows a timeline of advances that eventually led to the development of mRNA vaccines against COVID-19. The left column in Fig. III.2 follows advances in mRNA technology that allowed mRNA molecules to be injected into the cells of humans. The center column shows advances in lipid technology; these advances led to lipids that surrounded mRNA molecules and carried them into the body. The right column details advances in combining lipid molecules with modified mRNA, so that the combination could produce a vaccine that would be injected into the body and would stimulate the body’s cells to produce ‘spike’ proteins to combat the SARS CoV-2 virus. The far-right column gives a timeline of commercial efforts to produce a vaccine employing these mRNA and lipid nanoparticle techniques.
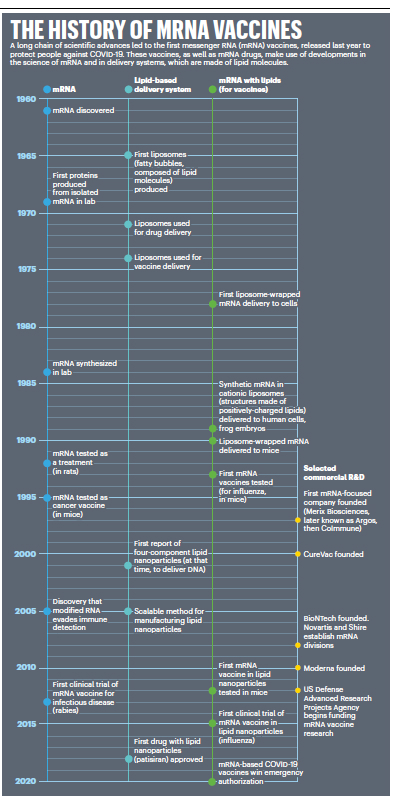
Figure III.2: A timeline of advances that led to the development of mRNA vaccines to deal with the SARS CoV-2 virus in 2020. Left column: advances in the use of mRNA to produce vaccines or treat diseases. Middle column: advances in development of lipids that carried the mRNA molecules into the cells of the body. Right column: combining the mRNA and lipid advances in order to produce vaccines. Far right column: timeline of commercial efforts to produce a vaccine employing mRNA and lipid nanoparticle techniques.
Figure III.3 is a schematic picture of an mRNA vaccine, in this case a vaccine against COVID-19. A molecule of mRNA is enclosed within a lipid nanoparticle. The mRNA contains the code for cells to produce the spike protein that is used by the SARS-CoV-2 virus to enter and infect cells. As we mentioned earlier, the mRNA molecule has been modified to replace the uridine nucleotide with pseudouridine. This was the advance discovered by Karikó and Weissman, and it prevents the mRNA from producing inflammatory reactions when it is injected into cells. The lipid nanoparticle that encases the mRNA is composed of four types of lipid molecules. One of them is ionizable, and initially it is positively charged. This increases the affinity of the lipid nanoparticle to the negatively charged mRNA molecule. But when the nanoparticles enter the bloodstream, the positive charge is turned off; this decreases toxic reactions of the LNPs with the body.
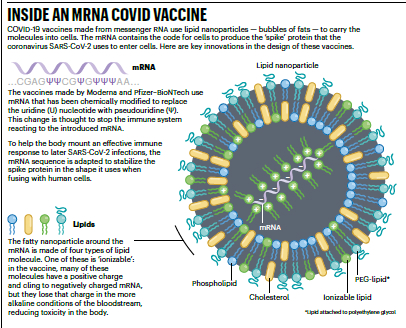
Figure III.3: Details of an mRNA COVID Vaccine. The messenger RNA is encased in a lipid nanoparticle that carries the mRNA into a cell. The mRNA contains the code that is used by cells to produce the spike proteins characteristic of the SARS CoV-2 virus. The mRNA has been modified to replace the uridine nucleotide with pseudouridine; this change apparently turns off the immune system reaction to the mRNA. One of the lipid particles in the fatty nanoparticle is ionizable; in the cell this makes the nanoparticle cling to negatively charged mRNA, but in the bloodstream the nanoparticles lose their charge.
mRNA vaccines have a unique mechanism of action, one that is quite different from normal vaccines. Figure III.4 shows the sequence of events for an mRNA vaccine against the SARS-CoV-2 virus. First, scientists generate an mRNA sequence which provides a blueprint for making the spike protein that is characteristic of the SARS-CoV-2 virus. That mRNA sequence is encased inside a lipid nanoparticle shown in Fig. III.3. When that mRNA vaccine is injected into the body’s muscle cells, the mRNA delivers the instructions to cells to make millions of copies of the spike protein. Those proteins are harmless but have identical features to those of the targeted virus (in the case of COVID, the spike proteins of the SARS-CoV-2 virus). When the instructions carried by the mRNA are decoded and the protein is assembled, our immune system is activated to produce antibodies. When a real virus with spike proteins enters the body, those antibodies will attack the virus.

Figure III.4: How an mRNA vaccine protects the body against the SARS-CoV-2 virus. First, an mRNA sequence is created that codes for the spike protein of the virus. The RNA sequence is encased in a lipid nanoparticle, and then injected into the body. The mRNA sequence stimulates cells to produce millions of copies of the harmless spike protein. The immune system produces antibodies that will attack when virus particles containing the spike protein enter the body.
After the antibodies have been created, the mRNA instructions break down. For a period of time, the immune system will ‘remember’ the spike protein; however, this memory diminishes over time, so a booster vaccine will be necessary to protect over the long run.
mRNA vaccines have many advantages over conventional vaccines.
- Conventional vaccines typically use either weakened or inactivated viruses. This could potentially lead to problems where a conventional vaccine would produce the virus it was supposed to attack. Such problems do not arise with mRNA vaccines, since they just provide our body with instructions for producing specific parts of a virus that are not capable of self-replication.
- All components of mRNA vaccines are identical except for the specific RNA sequence. As a result, mRNA vaccines can be produced in a small fraction of the time taken to produce a conventional vaccine.
- When a virus is spreading, it often mutates into a different form from the initial virus. Vaccines that were created to battle one specific virus may be ineffective against the mutant. However, when the SARS-CoV-2 virus mutated, new mRNA vaccines targeting the mutated form could be rapidly created.
- The ability of mRNA vaccines to be altered rapidly when a virus mutates should be particularly effective against seasonal flu epidemics. Every year researchers have had to guess in February or March which flu variant will be dominant in September, the beginning of the Northern Hemisphere flu season. Given the long lead time to develop them, conventional flu vaccines have to be formulated many months before the start of the flu season. In years when the flu virus variant differed from the one that the flu vaccine targeted, the flu vaccine was sometimes highly ineffective. But with the speed of development of mRNA vaccines, researchers could wait until June to see which flu strains are circulating in the Southern Hemisphere.
IV: The mRNA Vaccines and the COVID-19 Pandemic:
The COVID-19 pandemic proved to be the testing ground for mRNA vaccines. The vaccines were produced in record time under the Operation Warp Speed vaccine development of the first Trump administration. The mRNA vaccines developed by Pfizer/BioNTech and Moderna were approved by the FDA for emergency use in December 2020. Figure IV.1 shows U.S. COVID death rates by county. The counties are broken down by quintile; the five curves show death rates in counties representing segments of the population that voted for Trump or Biden in the 2020 presidential election. Bright red is the quintile with the highest percentage of Trump voters while bright blue represents counties with the highest Biden voters.
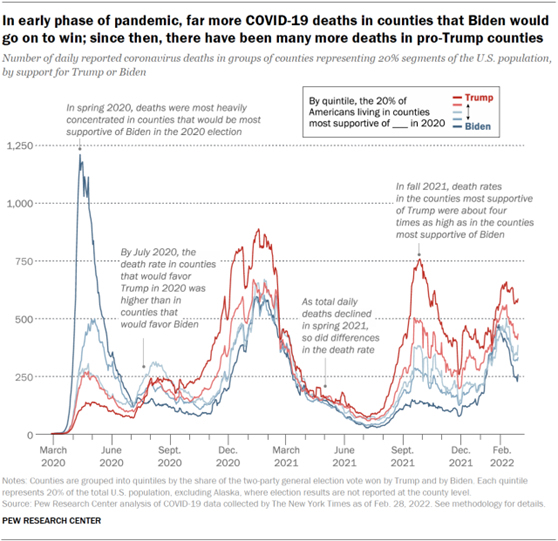
Figure IV.1: The COVID death rate from March 2020 to March 2022. Death rates are broken down by county. Dark red: highest quintile of votes for Trump in the 2020 national election; dark blue: quintile with highest percentage of votes for Biden. In the first half of 2020, COVID deaths were most concentrated in large urban areas that were strongly pro-Biden. Total deaths dropped rapidly in spring 2021 after the COVID vaccines were released. However, by fall 2021 death rates in counties most supportive of Trump were four times as high as in the counties with the highest percentage of Biden voters.
In the first half of 2020, before a COVID vaccine had been released, Fig. IV.1 shows a big spike in COVID-19 deaths in large urban areas where Biden votes were strongest. But by July 2020, COVID death rates were larger in counties that voted most heavily for Trump. With new variants of the SARS-CoV-2 virus appearing, COVID death rates increased rapidly. However, after the COVID vaccines were released in early 2021, death rates dropped precipitously for all groups. This shows the effectiveness of the mRNA vaccines. Around the world, it is estimated that the COVID vaccines saved 2.5 million lives.
The COVID-19 mRNA vaccines did not prevent all vaccinated people from contracting the disease. However, when a vaccinated person contracted COVID, they experienced a much milder form of the disease. The vaccine prevented most hospitalizations and deaths from the virus. It was also the case that when variants of the SARS-CoV-2 virus appeared, pharmaceutical companies were able to update the vaccines so that they targeted the most prevalent strain that was circulating.
Side effects of the mRNA vaccines were for the most part mild. Common effects were pain, soreness and redness at the injection site, fatigue, headache, muscle pain, joint pain, chills, fever, and nausea (particularly for the Moderna vaccine), all of which typically lasted for a day or two. There were also a few very rare and dangerous side effects.
- Anaphylaxis: this allergic reaction may require immediate treatment with an EpiPen. Anaphylaxis occurs in roughly 5 cases per million doses of the vaccine.
- Myocarditis (inflammation of the heart muscle) and Pericarditis (inflammation of the outer lining of the heart): in roughly 80% of these rare cases, patients had essentially completely recovered after three months. Also, myocarditis and pericarditis occurred much more frequently in unvaccinated people who contract COVID.
- Guillain- Barré Syndrome (GBS): this is a rare side effect. However, it was found that occurrences of GBS within three weeks of vaccination were 21 times higher for the Johnson & Johnson/Janssen non-mRNA COVID-19 vaccine than either the Pfizer/BioNTech or Moderna mRNA vaccines. After studying this for a couple of years, the Advisory Committee on Immunization Practices (ACIP) recommended discontinuing the J&J/Janssen vaccine; after May 2023 this vaccine was no longer available in the U.S.
- Thrombosis with Thrombocytopenia Syndrome (TTS): TTS causes blood clots and low platelet counts. It occurred in about 4 cases per one million doses, with somewhat higher rates among women 30 – 49. Again, it was found that TTS occurred more frequently with the J&J/Janssen vaccine than with Pfizer/BioNTech or Moderna.
To summarize, the mRNA vaccines used against the COVID pandemic had very few adverse reactions. The majority of adverse reactions were quite minor. There were some events of myocarditis or pericarditis, particularly among young men, but vaccine-related events were far fewer than myocarditis or pericarditis that resulted from an unvaccinated individual getting COVID.
As we will discuss in Section V of this post, social media was full of misinformation regarding the safety and effectiveness of the mRNA COVID vaccines. A major feature of these conspiracy theories reflected the political dimensions of anti-vaccine sentiment. After the COVID vaccines had been available to the public, there was extensive antipathy by Republicans to the vaccines. Donald Trump was a major influence in this hesitancy. As the 2020 election grew near, Trump claimed that the COVID-19 pandemic would “vanish” at any time. Republicans formed “medical freedom” groups that opposed vaccination mandates, masking requirements and prohibitions on gatherings of large groups.
A result was that while at least 80% of Democratic voters were getting the COVID vaccine, roughly half of Republicans were vaccinated. Figure IV.2 shows results for every county in the U.S. from May to December of 2021, a time when the COVID vaccines were readily available. The left-hand graph shows the percentage of adults who were vaccinated against COVID vs. the percent vote that Donald Trump received in that county in the 2020 national election. The black cross is the national average of vaccine acceptance, while the red cross shows the average among heavily Trump counties and the blue cross shows the average vaccinations among heavily Biden counties. The right-hand graph shows the number of COVID deaths per 100,000 inhabitants in each county, again plotted against the percentage of Trump voters in that county, with similarly colored crosses.
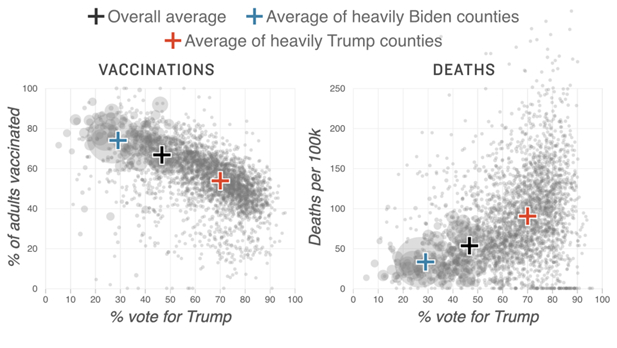
Figure IV.2: Left: percent of adults who were vaccinated against COVID from May to December 2021 by county, vs. percent of that county’s vote for Trump in the 2020 national election. Black cross: national average; red cross: average fraction of adult voters who were vaccinated in heavily Trump counties; blue cross: average fraction of voters who were vaccinated in heavily Biden counties. Right: COVID deaths per 100,000 inhabitants in each county vs. percent of that county’s vote for Trump. Black cross: national average; red cross: average of Trump counties; blue cross: average of Biden counties.
Each of the graphs in Fig. IV.2 can be represented by a straight line, with vaccinations decreasing steadily as the fraction of the vote to Trump increases. Also, the COVID death rate increases linearly with the percent vote for Trump in 2020. This is clearly the result of misinformation about the pandemic and about the mRNA vaccines which was accepted by Republican voters. The death rate in the counties with the highest 2020 vote for Trump was roughly six times higher than the death rate in counties with the lowest percentage vote for Trump. The association of COVID deaths with Trump supporters was stronger than any other causative factor.
To summarize, the mRNA vaccines used to fight COVID were quite exceptional. They were extremely effective in preventing hospitalization or death from COVID. Also, they had very small numbers of dangerous side effects. Finally, they could be produced rapidly, and new vaccines to combat variants of the SARS-CoV-2 virus could be very rapidly generated. As we will see in the following Section, the mechanism by which mRNA vaccines teach the immune system to recognize viruses or other disease molecules is novel and provides a promising method to fight other diseases. As a result, we would expect research on mRNA methods to comprise a major avenue to develop new products. This could lead to a “golden age” of new, effective and safe products that utilize mRNA techniques to produce vaccines and to develop new ways to combat diseases.
Alas, under the current Trump administration, we are seeing significant hostility to mRNA techniques. This stems from a regrettable combination of circumstances. Vaccines have been associated with products released under the Biden administration, and also were a major focus of Anthony Fauci’s research. The Trump administration is eager to wipe out any efforts supported by Biden; also, they seek retribution against anything associated with Fauci, at least in part because Fauci was seen as insufficiently loyal to Trump. In addition, Trump’s Secretary of Health and Human Services Robert F. Kennedy, Jr. is a bitter foe of Fauci because of RFK’s anti-vaccine ideology. Kennedy also stated without any basis in fact that the mRNA COVID vaccines were the most deadly vaccines in human history.
In May 2025, the National Institutes of Health cancelled research on mRNA vaccines, and announced a new program to create vaccines using the old inactivated whole-virus techniques rather than the far more promising mRNA methods. They named this effort Generation Gold Standard, in a completely ass-backwards claim that these whole-virus vaccine methods were the world’s best and most promising techniques. RFK, Jr. stated that “Every innovation in vaccine development must be grounded in gold standard science and transparency.” Typical of his vaccine denial, RFK’s claims are exactly the opposite of the facts with respect to vaccines. But what did our U.S. Senators expect when they confirmed as HHS Secretary a man who had been spreading lies about vaccines for the past 30 years?
V: Other Uses for mRNA Methods in Fighting Disease
The outstanding success of the Pfizer and Moderna mRNA vaccines against the SARS-CoV-2 virus, both of which by now have full approval from the U.S. Food and Drug Administration (FDA), has demonstrated the great effectiveness of mRNA vaccines. The approach of embedding mRNA synthesized to encode a specific protein within a lipid nanoparticle, like that illustrated in Fig. III.3, allows an mRNA vaccine to penetrate into the cytoplasm (but not the nucleus) of targeted cells. It is no surprise, then, that various pharmaceutical companies and the U.S. government have been working on the development of mRNA vaccines to address a variety of other diseases. A number of these efforts are currently being tested in clinical trials.
At least four different versions of an mRNA flu vaccine are currently in clinical trials. Moderna alone has five distinct mRNA flu vaccines in process. The one furthest along in Phase 3 (the final phase) clinical trials is a vaccine to improve the efficiency in preventing infections with influenza B strains that cause seasonal disease in humans. Pfizer has a single-dose mRNA flu vaccine that targets four different strains of the virus in Phase 3 clinical trials. That would represent a significant advance over current flu vaccines which need to be tailored each year to the best guess of the strains that will become dominant in the next flu season. There is currently no vaccine in trials that would address influenza A H5 strains, which can potentially cause pandemics. The H5N1 bird flu strain is considered to be the most immediate concern for the next pandemic. The Department of Health and Human Services (HHS) had $776 million contracts with Moderna to develop and test an mRNA vaccine that would address bird flu, but under the leadership of Robert F. Kennedy, Jr., who considers mRNA technology still untested, HHS has just canceled those contracts, causing significant jeopardy to Americans’ health.
mRNA vaccines offer new hope for AIDS. Despite numerous attempts, there has not yet been a successful vaccine to prevent the frequently mutating HIV virus, which causes AIDS. Both Moderna and the National Institute of Allergy and Infectious Disease (NIAID) have mRNA HIV vaccine candidates in Phase 1 trials.
Zika is a mosquito-borne virus that has mostly infected people in countries south of the U.S. However, ongoing climate change may cause the mosquito carriers to migrate northward. The virus is especially severe for pregnant women, since it can cause miscarriage, stillbirth, or birth defects. Moderna has an mRNA Zika vaccine candidate in Phase 2 clinical trials.
Other infectious diseases for which mRNA vaccines are currently in development include RSV (respiratory syncytial virus), which can be dangerous for older adults and babies, and CMV (cytomegalovirus), which can cause serious symptoms in people with weakened immune systems and in babies, who may suffer hearing loss.
Perhaps the most surprising application of mRNA vaccines currently under development addresses the treatment, rather than prevention, of various types of cancer. A sample of cancerous cells in a patient can reveal specific proteins that are found exclusively in those cells. An mRNA vaccine can then train the body’s immune system to recognize and destroy cells containing those proteins. An mRNA cancer vaccine thus provides a new form of immunotherapy that could be used in combination with other types of immunotherapy or with chemotherapy. Several of the mRNA developments under way provide personalized cancer vaccines, which target a patient’s particular tumor cells. mRNA cancer vaccines currently in clinical trial address various types of cancer: melanoma; solid tumors; non-small cell lung cancer; colorectal cancer; pancreatic cancer; and ovarian cancer.
In short, mRNA technology offers the promise now to transform the prevention and treatment of a variety of diseases that vary from dangerous to deadly for humans.
VI: Opposition to mRNA Methods
Despite the tremendous successes of mRNA vaccines in the fight against COVID, and the promise of mRNA products currently in development that would protect against many other diseases, social media is awash with criticism of mRNA products. Since almost all of these claims of harm from mRNA products are incorrect, we may inquire as to the motivation of those who disseminate them. Much of this criticism arises as an offshoot of politically inspired resistance to practices advocated in the pandemic. Right-wing “Medical freedom” groups strongly opposed mask mandates and vaccination requirements adopted during the COVID-19 pandemic. Despite the fact that the Operation Warp Speed push during the first Trump administration culminated in the COVID vaccines that incorporated mRNA techniques and saved millions of lives around the globe, Trump quickly began to dispute the severity of the pandemic and criticized public health recommendations for limiting the death and injury caused by the SARS-CoV-2 virus.
Public sentiment against vaccine requirements extended to claims that the mRNA techniques were flawed or dangerous. This was also amplified by conspiracy theories suggesting that the COVID crisis was either invented or over-hyped by Big Pharma companies (alternatively, by individual billionaires such as Bill Gates or George Soros, as shown by cartoons on social media sites in Figs. VI.1 and VI.2). As we demonstrated in earlier sections, the mRNA vaccines appear to be wonderfully safe and effective. The two researchers in Fig. III.1 who made seminal discoveries that led to the development of these mRNA products shared the 2023 Nobel Prize in Physiology or Medicine.

Figure VI.1: Conspiracy theory cartoon implying that Bill Gates is trying to infect a child with a spike protein (via an mRNA COVID vaccine).

Figure VI.2: Conspiracy theory cartoon implying that George Soros funded biological laboratories in order to manufacture and release the SARS CoV-2 virus.
Many of the anti-mRNA posts on social media simply repeat falsehoods that have arisen from other sources. However, there are a few major influencers who have been responsible for disseminating these lies to very large audiences. In this section, we provide capsule bios of four people who have been most vocal in spreading claims that mRNA techniques are inherently harmful. We also include a description of a bill that has been introduced into the Minnesota state House that would classify products utilizing mRNA techniques as “bioweapons of mass destruction.”
Robert F. Kennedy, Jr. RFK Jr., shown in Fig. VI.3, is currently the Secretary of Health and Human Services in the second Trump Administration. On Dec. 6, 2021 he testified at a Louisiana House meeting that was considering a bill that would require students to get vaccinated against COVID-19 before enrolling in school. He made a number of false or misleading claims about the COVID vaccines, most of which used mRNA methods. Kennedy stated that records of the vaccine confirmed that “this is the deadliest vaccine ever made.” Kennedy based his claim by comparing reports on the nation’s Vaccine Adverse Event Reporting System (VAERS), which include all self-reported adverse health episodes that occurred any time after receiving the vaccines. Based on those records, RFK Jr. stated that “more people who have died in eight months from this vaccine than from 72 vaccines over the last 30 years.”

Figure VI.3: Robert F. Kennedy Jr., the current Secretary for Health and Human Services. Kennedy is a conspiracy theorist and a vaccine denier.
But RFK’s claims were based on a mischaracterization of the VAERS system. This system allows anyone to upload claims regarding potential vaccine injuries. These claims are not screened in any way, so anyone can assert that any health issue was caused by a vaccine. As a result, the VAERS system has a disclaimer stating: “The number of reports alone cannot be interpreted or used to reach conclusions about the existence, severity, frequency, or rates of problems associated with vaccines.” Furthermore, VAERS reports “cannot be used to determine if a vaccine caused or contributed to an adverse event or illness.” Centers for Disease Control (CDC) spokesperson Martha Sharan stated that “Reports of adverse events, including deaths, do not necessarily mean that a COVID-19 vaccine caused a health problem. Statements that imply that reports of deaths to VAERS following vaccination equate to deaths caused by vaccination are scientifically inaccurate, misleading and irresponsible.”
Dr. Rebecca Weintraub, assistant professor in the Department of Global Health and Social Medicine at Harvard Medical School, observed that there exists data on billions of people who have received multiple doses of the COVID-19 vaccines. She said “We are confident that we have a robust database that these vaccines are as safe and effective as other vaccines. It prevents death, it prevents severe disease and it decreases transmission.” As an indication of the fact that the VAERS system might be abused by critics of the COVID vaccines, it was reported that claims of vaccine deaths on VAERS increased by 6,000% from the first quarter of 2020 to the first quarter of 2021, just after the COVID vaccines were released. After conducting an inquiry into health effects that might be caused by mRNA vaccines, Politifact rated Robert F. Kennedy, Jr.’s claim (that the COVID mRNA vaccines were the “most deadly” vaccines ever produced) as a “pants on fire” falsehood. If the COVID vaccines were as deadly as RFK claimed, one would expect the death rate to be much higher among vaccinated than unvaccinated individuals, while in reality it was an order of magnitude lower (see Fig. I.1).
Dr. Joseph Ladapo: Joseph Ladapo is a Nigerian-American physician who has been a constant source of misinformation regarding vaccines in general and COVID practices in particular. Ladapo, shown in Fig. VI.4, received both M.D. and Ph.D. degrees in Health Policy from Harvard University. He was later hired by the University of California, Los Angeles where he received tenure. In early 2020, Ladapo wrote a number of op-ed pieces for the Wall Street Journal about the COVID-19 pandemic. Despite the fact that he was not a specialist in infectious diseases, Ladapo touted unproven (and later shown to be ineffective) treatments for COVID, criticized mask mandates and other public-health measures taken by various authorities, and publicly questioned the safety of vaccines.

Figure VI.4: Joseph Ladapo, currently the Surgeon General of Florida. Ladapo has been responsible for promulgating a great deal of misinformation about vaccines and COVID practices.
Ladapo claimed that his comments were based on his experience treating COVID patients at UCLA; however, several of his UCLA colleagues stated that he had never treated any COVID patients. Ladapo’s comments caught the attention of Florida governor Ron DeSantis. In September 2021, Ladapo was appointed as Florida’s Surgeon General. At the same time, he was appointed as an Associate Professor at University of Florida Health. Notably, during his confirmation hearings in the Florida Senate, Ladapo’s former supervisor at UCLA said that Ladapo’s actions during the pandemic violated the Hippocratic Oath.
In October 2022, Ladapo suggested that men aged 18 to 39 should not be vaccinated. He based his advice on an “anonymous non-peer-reviewed analysis” that claimed men in this age range who received mRNA COVID-19 vaccines had very high numbers of cardiac-related deaths. In January 2023, the Faculty Council of the University of Florida College of Medicine concluded that Ladapo’s recommendation was based on “careless and contentious research practice.” It was claimed that Ladapo had personally altered the report; while the initial report concluded that COVID vaccines posed no significant risk for young men, Ladapo was said to have altered it to conclude that men age 18 -39 should not be vaccinated. However, this rebuke did not stop Ladapo from releasing misinformation about COVID and vaccines. In March 2023, both the Centers for Disease Control and the Federal Drug Administration publicly criticized Ladapo for issuing information that misinterpreted reports from the Vaccine Adverse Event Reporting System (VAERS).
In January 2024, Dr. Ladapo issued a statement that called for halting the use of all mRNA vaccines. He gave as his reason the possibility that small amounts of residual DNA contained in the mRNA vaccines could integrate into, and transform, human DNA. Ladapo stated “If the risks of DNA integration have not been assessed for mRNA COVID-19 vaccines, these vaccines are not appropriate for use in human beings.” Ladapo’s claim was assailed by many experts in vaccines. Dr. Paul Offit, director of the Vaccine Education Center at the Children’s Hospital of Philadelphia, said that “It’s virtually impossible for these DNA fragments to do any harm. They are clinically and utterly harmless. It is hard to believe that Dr. Ladapo actually issued that statement.” Dr. Eric Rubin, editor in chief of the New England Journal of Medicine, stated that for Dr. Ladapo’s claim to be true, humans would need to have an enzyme that would incorporate foreign DNA into their genomes. “We don’t have one,” said Rubin. “There is no mechanism and no credible evidence” for Ladapo’s comments.
Apparently, Dr. Ladapo’s concerns arose from a 2007 FDA document regarding DNA vaccines that contain plasmids. Ladapo incorrectly assumed that statements in this document referring to potential issues with DNA vaccines would also apply to mRNA vaccines. At present, there are no DNA vaccines on the market in the U.S. Ladapo criticized the CDC and FDA for not testing whether mRNA vaccines allow integration of foreign DNA into the DNA of vaccine recipients. “Their failure to test for DNA integration with the human genome – as their own guidelines dictate – when the vaccines are known to be contaminated with foreign DNA is intolerable,” Ladapo posted on X. However, mRNA vaccines are only inserted into the body of a cell, and not the nucleus. Foreign DNA would need to somehow get into the nucleus of a cell, and there is no evidence that this is occurring, and no known mechanism for how this would occur. Former senior FDA official Dr. Peter Marks said, “We now have access to global surveillance data on over one billion doses of the mRNA vaccines that have been given, and there is nothing to indicate harm to the genome.”
Joseph Ladapo continues to make incendiary claims regarding the safety and effectiveness of vaccines. His remarks polarize and politicize the issue of vaccine safety, particularly because his claims are absolutely unfounded. Dr. John Wherry, director of the Institute for Immunology at the University of Pennsylvania, categorized Ladapo’s statements as “very irresponsible. He has, however, demonstrated a tenuous grasp of science and medicine in general over the course of the pandemic, so this is not surprising.”
Robert Malone:
We came upon Robert Malone earlier in this post. Malone, shown in Fig. VI.5, was a graduate student at the Salk Institute who was involved in early discoveries regarding mRNA. As a result, Malone contends that he is the “inventor” of the mRNA vaccines. However, reporter Davey Alba wrote a New York Times article citing Malone’s co-workers as saying that “his role in its creation [of mRNA vaccines] was minimal at best.” Dr. Gyula Acsadi, a co-author of Malone’s on a 1990 paper showing that injecting RNA into muscle could produce proteins, says that Malone’s statement that he is the “inventor” of the mRNA vaccines is a “totally false claim.” At the start of the COVID-19 pandemic, Malone promoted famotidine, ivermectin and hydroxychloroquine as effective against the virus. In addition, he was criticized for making strong claims that the spike proteins generated by the mRNA vaccines were toxic. In fact, the mRNA vaccine uses the mRNA to make spike proteins in the patient’s cells. The cells then “show” the spike protein to the immune system. T cells in the immune system remember the spike protein. If a person is later exposed to the virus, the immune system recognizes and kills the infected cells. The spike protein produced by the mRNA does not kill cells in the body, nor is it carried by the bloodstream to other parts of the body. Roughly 1% of the vaccine reaches the bloodstream, where it is destroyed by liver enzymes.
Figure VI.5: Robert Malone. He was involved in early experiments with mRNA. However, he issued much misinformation about the COVID vaccines and is currently a prominent figure denying the safety and efficacy of mRNA vaccines.
Malone has continued to spread misinformation about mRNA techniques and about the COVID-19 vaccines that use mRNA techniques. In November 2021, Malone shared a video on Twitter regarding Jake West, a 17-year-old Indiana high school student who died from sudden cardiac arrest. The video claimed that West had died as a direct result of vaccination against COVID-19. Unfortunately for Malone, West had actually passed away in 2013 as a result of a heart condition that had gone undiagnosed. In December 2021, Malone appeared on the Joe Rogan podcast and claimed that because of the COVID pandemic, Americans were developing “mass formation psychosis.” However, that psychosis is not found in manuals listing mental disorders; social psychologist Steve Reicher states that this condition is “more metaphor than science, more ideology than fact.”
Robert Malone is a favorite of COVID conspiracy theorists because of his claim that he is the discoverer of mRNA techniques. He has issued posts and videos on social media, interviews with podcasters and appearances at anti-vaccine rallies to push ineffective medications against COVID and to make false statements claiming that the spike proteins produced by the COVID mRNA vaccines are cytotoxic. In April 2022, Malone claimed without citing any evidence that the COVID-19 vaccines were “causing a form of AIDS.” Virologist Dr. Angela Rasmussen maintains that Malone is peddling disinformation about COVID and the mRNA vaccines. “It’s extraordinarily dishonest and morally bankrupt,” she stated.
In June 2025, HHS Secretary Robert F. Kennedy, Jr. fired all 17 members of the Advisory Committee on Immunization Practices (ACIP); RFK Jr. claimed that all members of ACIP were guilty of “malevolent malpractice.” Kennedy’s claim that the ACIP members had conflicts of interest was deeply misleading. These committees have a number of rules regarding conflicts of interest and how to manage them, and it appears that all members of ACIP had both disclosed and managed potential conflicts. Two days after firing the ACIP members, Kennedy appointed 8 new members to this committee. One of them was Robert Malone. Note that Malone has his own potential conflicts of interest, as he received payments for serving as an expert witness in lawsuits that accused Merck of having defects in two of its vaccines. In a 2023 video, Malone claimed that mRNA vaccines for COVID-19 had no benefits for children; he also alleged that these vaccines would cause damage to children’s organs. We have seen no signs of such damage from the mRNA COVID vaccines.
Dr. Peter McCullough: Peter McCullough was a prominent physician who became an outspoken proponent of conspiracy theories about the COVID-19 pandemic, and about the mRNA vaccines developed to treat the SARS-CoV-2 virus. McCullough, shown in Fig. VI.6, was the Vice Chief of Internal Medicine at the Baylor University Medical Center and a professor at Texas A&M University. In January 2021, just after the first COVID vaccines were approved for emergency use, McCullough co-authored a paper in the American Journal of Medicine. This paper set out a protocol of medicines to treat COVID, which consisted of hydroxychloroquine, zinc lozenges, aspirin and antibiotics. The editors of that journal later commented “What seemed reasonable last summer based on laboratory experiments has subsequently been shown to be untrue.” However, McCullough was undeterred. He later insisted that ivermectin was an effective treatment for COVID, despite clinical trials that clearly showed ivermectin to be ineffective for COVID. McCullough criticized the medical community for advising against using ivermectin, “There’s a mass mentality of almost intentionally harming patients … There is a global collusion, specifically in U.S. hospitals, to cause as much harm and death as conceivable.”

Figure VI.6: Dr. Peter A. McCullough, a physician who has made unsupported allegations regarding the safety of COVID vaccines, and in particular mRNA vaccines.
McCullough claimed that the dramatic reduction in COVID deaths was not due to the mRNA vaccines, but to his own at-home treatment protocol for the virus. He stated that his treatment protocol “saved millions of lives, spared millions and millions of hospitalizations.” Regarding the COVID vaccines, McCullough claims that there are overwhelming statistics that show dangerous side effects, including death, from these mRNA techniques. He claimed that in some individuals the spike proteins that are stimulated by the vaccine will “ravage the body” wherever that protein is produced. McCullough predicted that these vaccines will produce epidemics of “local brain injury … myocarditis and cardiac injury … liver injury … lung injury … and kidney injury.” In fact, he predicted, the COVID vaccination campaign “Will go down in history as the biggest medical biological product safety catastrophe in human history, by far. There’s nothing close.”
McCullough’s wild claims have proved baseless. An analysis by a group in Israel comparing vaccine recipients with unvaccinated individuals found that the risk of dangerous side effects was much greater from a COVID infection than from the vaccine. And a study by the Sage Institute found that vaccine side effects were not only rare, but they were far less frequent than the same side effects suffered by people who contracted COVID. For example, myocarditis and pericarditis cases among male youth were more than 30 times more likely for COVID sufferers than for people who had received two doses of the mRNA vaccines, and blood clots were 200 times more prevalent for those contracting COVID than for those who received an adenovirus-vector vaccine.
As a result of Peter McCullough’s wild assertions about injuries from COVID mRNA vaccines, in January 2025 the American Board of Internal Medicine revoked his board certifications in both internal medicine and cardiovascular disease. McCullough is currently chief science officer of The Wellness Company. “The owner of that company was reported as having invested in an anti-vaccine dating site, and also launching a coffee brand for “anti-woke” consumers. The Wellness Company also sells a supplement called “Ultimate Spike Detox,” which costs $89.99 for 120 capsules.” So McCullough continues to double down on his debunked claims about the dangers of the mRNA vaccines. At the same time, he profits by hawking items that he claims will shield purchasers from the imaginary dangers of mRNA products.
Minnesota Republican Luddites: In April 2025, a group of eight Republican delegates in the Minnesota House of Representatives introduced a bill, HF3219 (see Fig. VI.7), that designated a number of medical treatments as “weapons of mass destruction.” If this bill were passed, then possessing or administering such medical treatments would be a crime punishable by up to 20 years in prison. A specific target of this bill would be any treatments that employed messenger RNA (mRNA) techniques. So this bill was aimed at several of the COVID-19 vaccines. Those vaccines have saved millions of lives and are considered one of the most important medical and public health achievements of the 21st century.

Figure VI.7: A screenshot of the beginning of Minnesota House Bill 1319, which would declare health products containing mRNA to be “biological weapons of mass destruction,” and would make anyone possessing or administering such products subject to 20 years in prison.
The wording of this bill was essentially copied from claims by Joseph Sansone, a Florida psychotherapist who specializes in hypnotic methods. Sansone is a conspiracy theorist who claims that mRNA treatments consist of “nanoparticle injections” that amount to “biological and technological weapons of mass destruction.” Sansone specifically claims falsely and outlandishly that “more Americans have died from mRNA injections than in WWI, WWII, and the Vietnam War combined.” (Incredible hyperbole seems to be a characteristic of medical conspiracy theorists.) Apparently the bill introduced by the Republican congressmen has essentially zero chance of passage in the state of Minnesota. However, it is rather amazing that Republicans would sponsor such a bill in the state that is the home of the Mayo Clinic, which has conducted groundbreaking research on mRNA techniques, and whose research in this area would be criminalized under the proposed bill.
But this proposed bill did not stop with outlawing mRNA techniques. It also would prohibit “nanotechnology or nanoparticles that alter genes and create a biosynthetic cell replication;” presumably this would ban medical technologies like CRISPR. The bill would also ban “any human gene therapy product for any infectious disease indication.” This leads to the bizarre possibility that, if the bill somehow passed, Minnesota state authorities would presumably prosecute doctors and researchers who used these techniques under “weapons of mass destruction” statutes.
The Minnesota bill is an extreme example, but several other states are currently considering bills banning or limiting the use of mRNA techniques. An Idaho bill that would have paused all use of mRNA vaccines has not advanced, but already one regional health department in the state has stopped administering mRNA COVID vaccines. An Iowa bill initially proposed penalties for administering mRNA vaccines. A similar bill introduced in Montana has not advanced. Meanwhile, in Florida Governor DeSantis, no doubt advised by Joseph Ladapo, has called for a permanent ban on mRNA vaccine mandates. When politicians follow conspiracy theorists and people with minimal understanding of science, rather than the consensus of medical opinion and the overwhelming epidemiological evidence, Americans’ health is seriously jeopardized.
VII: Summary
The COVID-19 pandemic provided a worldwide emergency deadline to bring decades of biomedical research into mRNA vaccines to fruition. Despite what any denier may tell you, the Pfizer and Moderna COVID vaccines were enormous successes, saving as many as 2.5 million lives worldwide while inducing only mild side-effects in the great majority of people who received the vaccine. Serious side-effects were very rare and, in many cases, much less frequent than the same side-effect that would result from a COVID infection. As we have explained in detail in a previous post, the development of vaccines has been one of the great triumphs of modern science. The technology that led to mRNA vaccines represents a highly significant new breakthrough with many important potential applications in preventing and treating other diseases.
The messenger RNA in a vaccine is synthesized to produce specific proteins that allow the immune system to recognize potential incoming pathogens – viruses, bacteria, or fungi – or even tumorous cells. The mRNA is distinct from the pathogenic RNA that replicates itself inside the host body and causes infections. The spike proteins associated with the SARS-CoV-2 virus, for example, are harmless in a human body unless those proteins surround viral RNA and allow it to enter host cells. Thus, the COVID mRNA vaccines train the immune system to attack the virus without ever having to introduce the viral RNA in the body in the first place. The same technique can be used to address SARS-CoV-2 variants or other infectious disease pathogens by altering the synthesis of the mRNA molecule. Clinical trials are currently under way for a number of other mRNA vaccines that would address other infectious diseases or offer new immunotherapy treatments for cancer. Furthermore, the mRNA delivered in a vaccine is surrounded by lipids that allow it to enter the cytoplasm of a host cell – where protein production takes place – but not the nucleus of the cell, where the host’s DNA is stored. Hence, worries and false claims that the mRNA in a vaccine can alter a patient’s own DNA are baseless.
The demonization of mRNA vaccines that is being promoted by a few conspiracy theory influencers – unfortunately including the current U.S. Secretary of Health and Human Services – and spread by right-wing media and social media is tragic. It brings to mind the uninformed 18th– and 19th-century campaigns against vaccines to cure such diseases as smallpox. The Donald Trump administration in the U.S. is emboldening such science deniers and leading several Republican-led states to introduce legislation to ban or restrict mRNA vaccines. Such policies play on unfounded fears and jeopardize citizens’ health. We have pointed out in an earlier post how policies pursued by a number of Republican-led states are already contributing to an American mortality gap, in which Republican voters have significantly shorter life expectancy than their Democratic counterparts. The clinical trial protocols that have led to robust testing of many successful medical treatments and preventive measures work well. In order to let them work for new mRNA vaccines, it is likely that RFK, Jr. would have to be replaced as HHS Secretary with someone who actually understands science.
Source Material:
COVID-19 Pandemic: Our World in Data https://ourworldindata.org/coronavirus
The Fastest Vaccine in History, UCLA Health https://www.uclahealth.org/news/article/the-fastest-vaccine-in-history
Will Robert F. Kennedy, Jr. Make America Healthy Again? Not On Your Life, Debunking Denial Dec. 10, 2024 https://debunkingdenial.com/will-rfk-j-make-america-healthy-again-not-on-your-life/
States Echo RFK Jr. Agenda in Push for Ban on Vaccine Mandates, Bloomberg Law, https://news.bloomberglaw.com/health-law-and-business/states-echo-rfk-jr-agenda-in-push-for-ban-on-vaccine-mandates
US Cancels More Than $700 Million For Moderna Bird Flu Vaccine, Patrick Wingrove, Reuters, May 29, 2025 https://www.reuters.com/business/healthcare-pharmaceuticals/us-cancels-more-700-million-funding-moderna-bird-flu-vaccine-2025-05-28/
Eukaryote, Brittanica.com https://www.britannica.com/science/eukaryote
Messenger RNA, Wikipedia https://en.wikipedia.org/wiki/Messenger_RNA
The Tangled History of mRNA Vaccines, Elie Dolgin, Nature News Sept 14, 2021 https://www.nature.com/articles/d41586-021-02483-w
The Power of mRNA, Moderna, https://www.modernatx.com/en-US
COVID-19 mRNA Vaccine, COMIRNATY https://www.comirnatyhcp.com/
Global Estimates of Lives and Life-Years Saved by COVID-19 Vaccination During 2020 – 2024, J.P.A. Ioannides et al., MedRXiv.org Nov. 4, 2024 https://www.medrxiv.org/content/10.1101/2024.11.03.24316673v1.full
FDA Approves and Authorizes Updated mRNA COVID-19 Vaccines to Better Protect Against Currently Circulating Variants, FDA.gov Aug. 22, 2024 https://www.fda.gov/news-events/press-announcements/fda-approves-and-authorizes-updated-mrna-covid-19-vaccines-better-protect-against-currently
Coronavirus Disease 2019 (COVID-19) Vaccine Safety, CDC.gov, Jan. 31, 2025 https://www.cdc.gov/vaccine-safety/vaccines/covid-19.html
Pro-Trump Counties Now Have Far Higher COVID Death Rates. Misinformation Is To Blame, Daniel Wood, NPR Dec. 5, 2021 https://www.wgbh.org/news/national/2021-12-05/pro-trump-counties-now-have-far-higher-covid-death-rates-misinformation-is-to-blame
HHS, NIH Launch Next-Generation Universal Vaccine Platform for Pandemic-Prone Viruses, US Dept. of Health and Human Services, May 1, 2025 https://www.hhs.gov/press-room/hhs-nih-announces-generation-gold-standard.html
More Than COVID-19: 6 Other Promising mRNA Vaccines in the Pipeline, Alyssa Billingsley, GoodRX, June 16, 2023 https://www.goodrx.com/health-topic/vaccines/other-mrna-vaccines
Moderna Announces Clinical and Program Updates at 4th Vaccines Day, April 11, 2023 https://www.accessnewswire.com/748485/Moderna-Announces-Clinical-and-Program-Updates-at-4th-Vaccines-Day
Pfizer Initiates Phase-3 Study of mRNA-Based Influenza Vaccine, Sept. 15, 2022 https://www.pfizer.com/news/press-release/press-release-detail/pfizer-initiates-phase-3-study-mrna-based-influenza-vaccine
HHS Cancels $766 Million in Moderna Contracts for Vaccines for Flu Pandemics, Helen Branswell and Matthew Harper, Stat News May 28, 2025 https://www.statnews.com/2025/05/28/moderna-flu-vaccine-development-cancelled-by-hhs-mrna-platform-offers-speedy-pandemic-response/
What is HIV? Your GoodRX Guide, Shiv Sudhakar, Mar. 10, 2025 https://www.goodrx.com/conditions/hiv
Wikipedia, Zika Virus https://en.wikipedia.org/wiki/Zika_virus
Childhood RSV: Your GoodRX Guide, Patricia Pinto-Garcia, Oct. 8, 2024 https://www.goodrx.com/conditions/childhood-rsv
About Cytomegalovirus, CDC.gov, Jan. 17, 2025 https://www.cdc.gov/cytomegalovirus/about/?CDC_AAref_Val=https://www.cdc.gov/cmv/overview.html
Immunotherapy, American Cancer Society, https://www.cancer.org/cancer/managing-cancer/treatment-types/immunotherapy.html
The Disinformation Dozen: Source of Lies About COVID Vaccines, Debunking Denial Aug. 30, 2021 https://debunkingdenial.com/the-disinformation-dozen-source-of-lies-about-covid-vaccines/
Nobel Prize in Physiology or Medicine 2023, https://www.nobelprize.org/prizes/medicine/2023/summary/
Robert F. Kennedy, Jr. Wikipedia https://en.wikipedia.org/wiki/Robert_F._Kennedy_Jr.
“The COVID-19 Vaccine is the “Deadliest Vaccine Ever Made,” Sarah Putterman, Politifact.com, Dec. 10, 2021 https://www.politifact.com/factchecks/2021/dec/10/robert-f-kennedy-jr/no-covid-19-vaccine-not-deadliest-vaccine-ever-mad/
Vaccine Adverse Event Reporting System, HHS.gov https://vaers.hhs.gov/data.html
Joseph Ladapo Wikipedia https://en.wikipedia.org/wiki/Joseph_Ladapo
June 2025: Understanding Recent Announcements About COVID-19 Vaccines, Dr. Paul Offit, Vaccine Education Center, Children’s Hospital of Philadelphia, https://www.chop.edu/vaccine-education-center
Citing Misinformation, Florida Health Official Calls For Halt to COVID Vaccines, Apoorva Mandavilli, New York Times, Jan. 3, 2024 https://www.nytimes.com/2024/01/03/health/covid-vaccines-florida.html
Robert W. Malone Wikipedia https://en.wikipedia.org/wiki/Robert_W._Malone
The Latest COVID Misinformation Star Says He Invented The Vaccines, Davey Alba, New York Times Apr. 3, 2022 https://www.nytimes.com/2022/04/03/technology/robert-malone-covid.html
Fact Check: COVID-19 Vaccines Are Not ‘Cytotoxic’, Reuters Fact Check https://web.archive.org/web/20210725225335/https:/www.reuters.com/article/factcheck-vaccine-cytotoxic-idUSL2N2O01XP
Who is on RFK Jr’s New Vaccine Panel – And What Will They Do? Heidi Ledford and Rachel Fieldhouse, Nature News June 12, 2025 https://www.nature.com/articles/d41586-025-01852-z
Peter A. McCullough Wikipedia https://en.wikipedia.org/wiki/Peter_A._McCullough
COVID Vaccine Much Safer Than Catching the Virus, Study in Israel Finds, Maggie Fox, CNN Health, Aug. 25, 2021 https://www.cnn.com/2021/08/25/health/vaccine-risks-infection-comparison/index.html
Vascular Disease Patient Information Page: Vascular Considerations With COVID-19 Vaccines, A.L. Solomon et al, Society For Vascular Medicine Dec. 22, 2021 https://journals.sagepub.com/doi/10.1177/1358863X211066128
ABIM Revokes Certification of Another Doctor Who Made Controversial COVID Claims, Kristina Fiore, Medpage Today Jan. 2, 2025 https://www.medpagetoday.com/special-reports/features/113624
MN Republicans Introduce Vaccine Criminalization Bill Drafted by Florida Hypnotist, Christopher Ingraham, Minnesota Reformer Apr. 22, 2025 https://minnesotareformer.com/2025/04/22/mn-republicans-introduce-vaccine-criminalization-bill-drafted-by-florida-hypnotist/
Minnesota Legislature Bill HF3219, Office of the Revisor of Statutes, https://www.revisor.mn.gov/bills/bill.php?b=House&f=HF3219&ssn=0&y=2025
Lives Saved By COVID-19 Vaccines, PubMed Central, Sept. 20, 2022 https://pmc.ncbi.nlm.nih.gov/articles/PMC9537923/
Mind Matters and Everything Else With Dr. Joseph Sansone, Apr. 11, 2025 https://josephsansone.substack.com/p/breaking-mrna-mrna-bioweapons-prohibition
CRISPR, Gene Editing, and Beyond, Stanford Explainer: June 10, 2024 https://news.stanford.edu/stories/2024/06/stanford-explainer-crispr-gene-editing-and-beyond
Vaccine Makers Face mRNA Backlash as States Seek Further Restrictions, Amy Baxter, PharmaVoice, Mar. 19, 2025 https://www.pharmavoice.com/news/vaccine-mrna-backlash-state-restrictions-trump-rfkjr/742857/
Vaccinations, Debunking Denial, July 11, 2018 https://debunkingdenial.com/vaccinations-part-i/
Live Free AND Die: Why Republican Voters Are Dying Younger Than Democratic Voters, Debunking Denial, Apr. 18, 2025 https://debunkingdenial.com/live-free-and-die-why-republican-voters-are-dying-younger-than-democratic-voters/
