
October 12, 2025
Note: A number of acronyms that may not be familiar to all readers are introduced and explained the first time they appear in this post. But for the reader’s convenient reference, we include a glossary of all the acronyms here.
ADDM: Autism and Developmental Disabilities Monitoring Network, part of CDC
ADHD: Attention Deficit/Hyperactivity Disorder
ADOS-2: Autism Diagnostic Observation Schedule
ASD: Autism Spectrum Disorder
CDC: The U.S. Centers for Disease Control and Prevention
CHD8: A gene involved in chromatin remodeling, important for brain development
CRS: Congenital Rubella Syndrome
DSM: Diagnostic and Statistical Manual of Mental Disorders
FDA: U.S. Food and Drug Administration
HHS: U.S. Department of Health and Human Services
ID: Intellectual disability
IDEA: Individuals with Disability Education Act
KFF: Kaiser Family Foundation
LD: Learning disability
MAGA: Donald Trump’s “Make America Great Again” coalition
MMR: Measles-Mumps-Rubella vaccine
NAc: Nucleus accumbens, a brain section involved in the brain’s reward circuit
NDD: Neurodevelopmental disorders
NIH: National Institutes of Health
PDD-NOS: Pervasive development disorder, not otherwise specified
RRB: Restricted and repetitive interests and behaviors
SHANK3: A gene involved in the structure and function of synaptic junctions in neurons
VTA: Ventral Tegmental Area, a brain section involved in the brain’s reward circuit
I. introduction
On Sept. 22, 2025 Donald Trump and Robert F. Kennedy, Jr. announced that the use of Tylenol (acetaminophen) by pregnant mothers is a substantial cause of autism in children. This claim is unsupported by the full body of research on the subject, but that has never stopped either Trump or Kennedy from making false claims in the past. Trump, of course, loves to take credit for solving problems he doesn’t understand. After urging pregnant women to avoid using Tylenol, without appreciating the potential risks in following that advice, Trump said: “I always had very strong feelings about autism,” which he characterized as “among the most alarming public health developments in history.” It is quite possible that he doesn’t even understand that his policies have often tried to deny the very existence of many people on the autism spectrum, many of whom claim non-traditional gender identities.
RFK, Jr. has been obsessed about autism for many years. He became a leader of efforts to claim a link between vaccines – particularly, the measles-mumps-rubella (MMR) vaccine – and autism in 2005, convinced by a 1998 article in The Lancet by Andrew Wakefield, which was later retracted and judged fraudulent, and by mothers of autistic children. Very large epidemiological studies have demonstrated beyond any doubt that there is no such statistically significant link. Nonetheless, as Secretary of Health and Human Services (HHS), RFK, Jr. announced in March a new study to be carried out by the Centers for Disease Control and Prevention (CDC) to reconsider the link between vaccines and autism, with a prominent role to be played by David Geier, an author of several discredited articles claiming just such a link.
In an April press conference, Kennedy called the rapid rise in diagnosed autism cases an “epidemic” caused by “an environmental toxin” in which fully functional children had “regressed … into autism when they were 2 years old. And these are kids who will never pay taxes, they’ll never hold a job, they’ll never play baseball, they’ll never write a poem, they’ll never go out on a date. Many of them will never use a toilet unassisted.” These remarks demonstrated how little Kennedy understands about the conditions currently diagnosed as falling within the Autism Spectrum Disorder (ASD). First of all, the term “epidemic” is usually reserved in a medical context for infectious diseases that spread rapidly by person-to-person transmission, which is not at all the case for autism. Secondly, there is no evidence that children “regress” into autism; diagnosis often begins about 2 years of age and in most cases pediatricians find that children display behavior consistent with autism before it is diagnosed. And finally, Kennedy’s characterization of kids “who will never pay taxes,…” applies to a small fraction of diagnosed ASD children. Indeed, many currently diagnosed with ASD will become not only functional, independent adults, but ones who work, pay taxes, get married, and have children of their own.
Kennedy’s first instinct is to blame pharmaceutical companies for whatever diseases or disorders catch his attention, and he seldom makes it past his first instinct. Thus, having failed to establish a link between vaccines and autism, he now claims on the basis of a few studies, but not at all most robust epidemiological studies, that it is prenatal acetaminophen that causes autism. We will see in this post that the largest clinical studies refute this claim. While our understanding of autism is still evolving, it is clear that there is no simple single cause, and that genetic predisposition – never mentioned positively by Kennedy — is an important factor in determining who may fall on the autism spectrum.
What is driving Kennedy and Trump is the alarming rise in diagnosed cases seen in Fig. I.1. In 1970, only one in 10,000 U.S. children were diagnosed with autism. By 1999, the prevalence had grown to 1:500 and by 2022 (as reported by CDC in April 2025) the prevalence was 1:31. In interpreting that rise, however, it is critical that one take into account that the understanding of autism and its relation to and overlap with a number of other childhood developmental disorders, as well as the criteria used to diagnose autism, were also advancing rapidly over the past half-century. We have annotated Fig. I.1 with arrows indicating three editions of the Diagnostic and Statistical Manual of Mental Disorders (DSM) and other changes to autism diagnostic criteria. Comprehensive screening for autism has become much more common over this same period. Furthermore, public understanding and acceptance for people on the autism spectrum has also grown rapidly as information available on the internet, mutual support groups for autistic people and their families, and special educational opportunities have all expanded. These factors make it challenging to deduce how much of the rise in Fig. I.1 represents an actual increase in autism prevalence, as opposed to an increase in autism recognition.

Autism is hardly the only neurological condition whose understanding and diagnostic protocols have changed rapidly over the past several decades. The same caveats about changing diagnoses and public awareness could be raised about Alzheimer’s disease, for example. The overall prevalence of Alzheimer’s is increasing rapidly (see Fig. I.2), primarily due now to the increasing fraction of the U.S. population above 65 years of age, but changing diagnostics also have influenced the historical trend. Yet another set of neurological conditions that appears to have rapidly increasing prevalence are cases of gender dysphoria or gender identity in tension with sex assigned at birth. In all these cases observers would be well advised to exercise caution in interpreting the diagnosed or even self-reported prevalence, as our understanding of neurological development in fetuses, infants, children, and even seniors is rapidly advancing.

In Section II of this post we describe how the diagnosis of autism and related neuro-developmental disorders has changed over the years, the present understanding of the autism spectrum, and other factors that may influence the growing prevalence of the diagnosis. In Section III we consider historical attempts to blame the occurrence of autism on “cold” mothers and Trump and Kennedy’s new attempt to blame pregnant women who use acetaminophen to manage pain. Robust data refute both of those attempts to blame the mother. They also refute any significant role of vaccines in causing autism, as we discuss in Section IV. Section V discusses what we do know about causes of autism, especially the role of genetics and fetal brain development, and the correlations with non-traditional gender identities. We summarize in Section VI to demonstrate pointedly that Trump and Kennedy are leading people astray with their pronouncements.
II. is there really an “autism epidemic”?
Figure II.1 provides a schematic illustration of how the diagnoses of various neuro-developmental conditions have changed during the 20th and 21st centuries, including how several conditions formerly treated as independent have been merged under the umbrella of autism spectrum disorder (ASD).
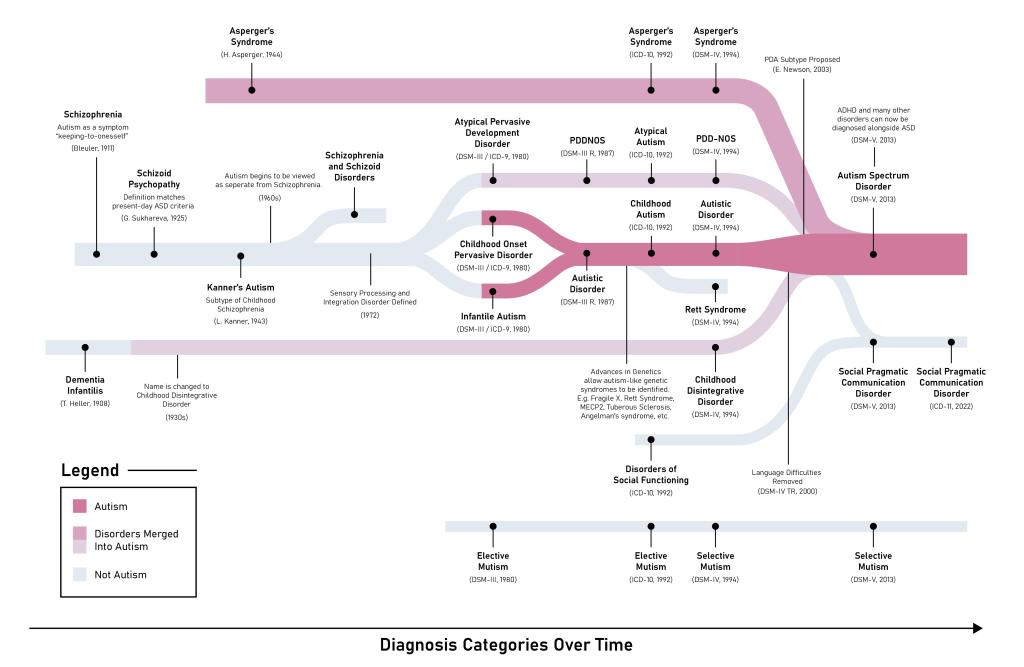
The modern treatment of autism began in 1943 when Leo Kanner described 11 children he had treated with “inborn autistic disturbances” featuring problems in social interactions and connectedness starting from birth and a resistance to change or insistence on sameness in their behaviors and surroundings. Almost simultaneously, in 1944, Hans Asperger defined a childhood syndrome he had observed in Austria, similar to Kanner’s autism but with less severe language and cognitive difficulties. Asperger’s syndrome and autism remained independent diagnoses until they were finally merged into the autism spectrum disorder in DSM-V in 2013.
Kanner viewed autism as a type of childhood schizophrenia, but beginning in the 1960s it was viewed as distinct from schizophrenia. In 1980 the third edition of the Diagnostic and Statistical Manual (DSM-III) separated childhood developmental issues into three distinct categories: infantile autism, childhood onset pervasive disorder, and atypical pervasive development disorder. The first two of these were subsequently recombined as autistic disorder in a 1987 update to DSM-III, while the third remained a distinct diagnosis (pervasive development disorder, not otherwise specified, or PDD-NOS) through DSM-IV, as did childhood disintegrative disorder. All of these, along with Asperger’s, were finally combined into autism spectrum disorders in DSM-V. Before DSM-V other common childhood diagnoses of ADHD (attention-deficit/hyperactivity disorder) and intellectual disability (ID) were viewed as independent of autism; one could diagnose one or the other, but not simultaneously with autism. That also changed with DSM-V, where it was understood that some children on the autistic spectrum could also be characterized as suffering from ADHD or ID.
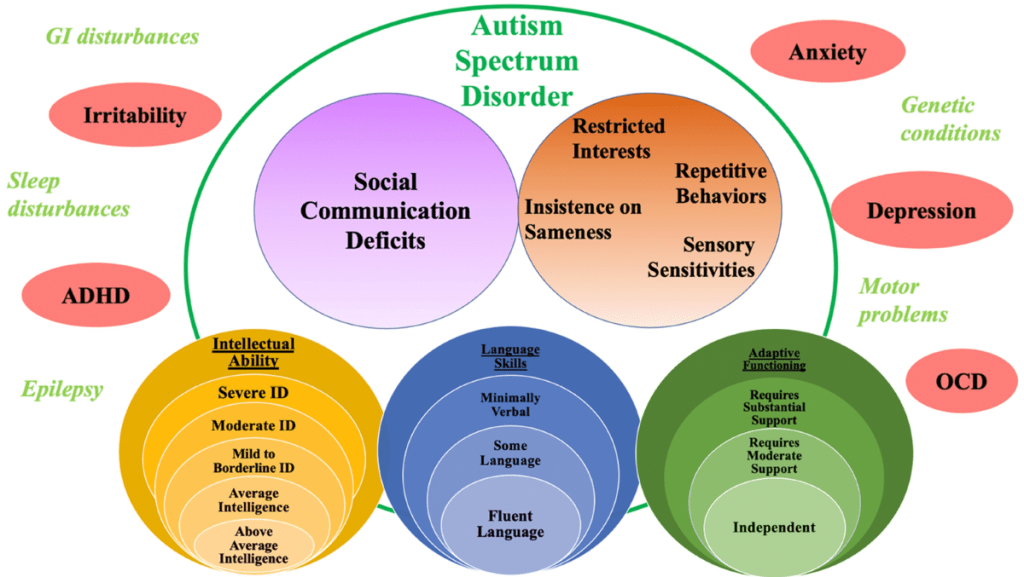
The current understanding of the broad autism spectrum disorder is then summarized in Fig. II.2. According to DSM-V the diagnosis of ASD depends on two core domains of symptoms. The social communication domain (purple circle in Fig. II.2) includes difficulties in both communication, social interaction, and interpreting social cues. The restricted and repetitive interests and behaviors (RRB) domain (brown circle in Fig. II.2) includes also a child’s insistence on sameness in behavior and environment and sensory sensitivities, such as oversensitivity to bright lights, loud noises, or strong smells. As indicated in the circles at the bottom of Fig. II.2, the autistic spectrum is now understood to encompass children with a very wide range of intellectual abilities – from severe disability to high but often narrowly focused intelligence – and language skills. There are three recognized levels of adaptive functioning and support needs, which are further elucidated in Fig. II.3.

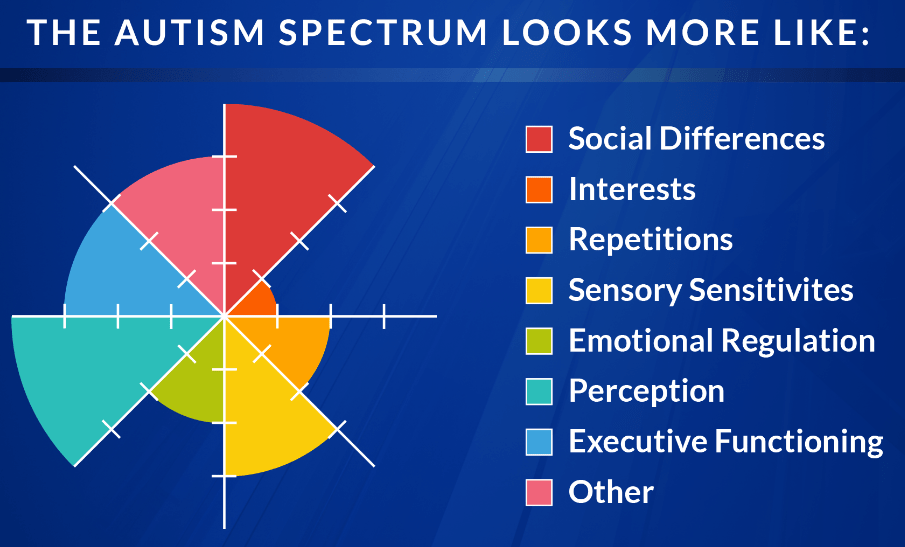
The symptoms of each person diagnosed with autism spectrum disorder are often characterized by an ASD wheel such as the one in Fig. II.4. Each sector of this wheel represents one set of typical ASD symptoms. A sector filled to the outer circumference of the circle represents neurotypical functioning with respect to that characteristic. In contrast, the smaller the radius to which the sector is filled, the more severely atypical the behavior. The filling of sectors will thus differ from individual to individual. In current diagnoses, ASD is meant to encompass such a wide variety of symptoms that it includes the world’s richest man, Elon Musk, the Oscar-winning actor Anthony Hopkins, and young climate activist Greta Thunberg at the high-functioning end.
The broadening of the autism diagnosis over time is certainly responsible for a large part of the rapid apparent growth in autism prevalence seen in Fig. I.1. For example, a 2019 review about distinguishing intellectual disability (ID) from ASD extended a 2015 analysis of children in special educational classes. The 1990 Individuals with Disabilities Education Act (IDEA) ensured that children with disabilities would have access to a free public education tailored to their special needs. The U.S. Department of Education maintains statistics on the numbers of children enrolled in these special classes with each type of covered disability. Figure II.5 shows the trend from 2000 to 2014 in children diagnosed with either ID or ASD. The trends make it clear that at least 40% of the rise in autism diagnoses among these special education students can be attributed to the decline in ID diagnoses, as children formerly diagnosed solely with ID more recently have often been diagnosed as autistic with an intellectual disability, corresponding to the upper regions of the yellow circles in Fig. II.2. A similar conclusion was reached in a study of ASD and ID prevalence in Atlanta between 1991 and 2010.

A study in Denmark found that 60% of the increase in autism prevalence in that country from 1980 to 1991 could be attributed to “the change in diagnostic criteria and the inclusion of outpatient contacts.” And those results were obtained before Asperger’s syndrome and PDD-NOS were folded into ASD diagnoses and before ADHD and ASD were allowed to be diagnosed together. The merging of Asperger’s with autism added many people without severe intellectual or language disabilities to the ASD count. Furthermore, a 2016 analysis found that “15-25% of youth with ADHD meet the criteria for ASD, whereas 50-70% of those with ASD have comorbid ADHD.” Thus, the incorporation of ID, ADHD, PDD-NOS, and Asperger’s within the autism spectrum most likely account for the majority of the increased prevalence of autism during the 21st century.
An additional significant contribution to the rise in autism prevalence comes from the introduction of more comprehensive screening. In 2007 the American Academy of Pediatrics recommended “universal autism screening during well-child visits at 18 and 24 months.” Many American parents have furthermore proactively sought autism testing for children whom they suspected would need access to special educational services. Still, the vigorousness in pursuing universal early autism testing varies significantly with location within the U.S. Figure II.6 shows the prevalence of ASD in 2022 among the sixteen U.S. monitoring stations of the Autism and Developmental Disabilities Monitoring (ADDM) Network. While 1 in 31 8-year old children were found to have ADS when averaged over the entire country, that ratio varied from 1 in 103 in Texas-Laredo to 1 in 19 in California. The Centers for Disease Control and Prevention attributes those differences to differences in evaluation and testing practices among the locations. For example, California has invested in comprehensive autism testing available at Regional Centers, including “assessing a child in multiple areas, such as communication, social skills, behavior, motor skills, and ability to complete daily tasks. An evaluation often includes interviews with the family, gathering medical and developmental history, observation and use of formal screening tools such as the ADOS-2. Research shows that identification and intervention lead to positive outcomes later in life for people with Autism.”
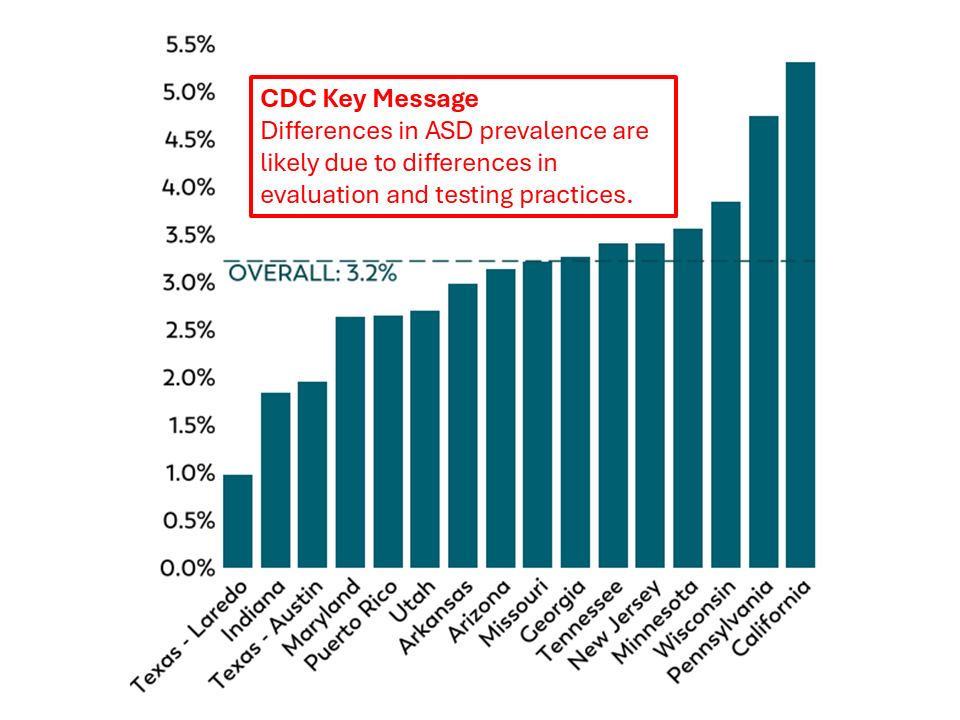
The differences in Fig. II.6 suggest that as comprehensive early screening is adopted more widely the apparent incidence of autism will grow further. A similar suggestion is offered by considering the fact that today ASD is diagnosed 3-4 times as frequently for boys than for girls. But changes that come from more comprehensive testing are improvements in recognizing children who fall somewhere on the broad autism spectrum; they do not indicate that the condition itself is becoming more widespread.
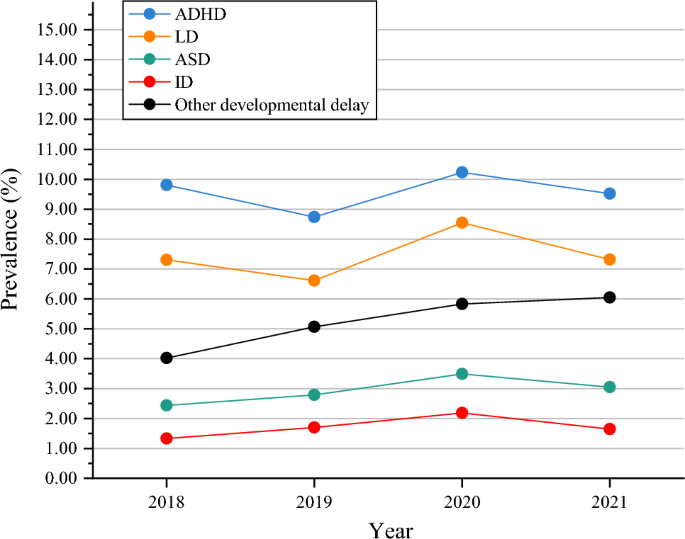
If an incidence rate of 3% or more for ASD among U.S. children seems alarmingly high, it is useful to consider the diagnosis in the context of incidence rates for other, sometimes overlapping, developmental disorders. A 2023 study investigated the prevalence of various developmental disabilities among U.S. children and adolescents, ages 3 to 17, during the years 2018-2021. The study’s results, shown in Fig. II.7, are based on data for 26,422 individuals available from annual National Health Interview Surveys. The categories in Fig. II.7 are not mutually exclusive; indeed, a fair fraction of the surveyed individuals have been diagnosed with two or even three of the conditions. But the overall prevalences of ADHD, learning disabilities, and other developmental delays are all significantly higher than that of ASD. Our understanding of neurodevelopmental anomalies is still at an early stage, but we have to come to terms with the fact that more than a tenth of American children are afflicted with them. And it does not appear from worldwide data that the U.S. is an outlier in this percentage.
Additional contributions to the apparent increase in autism prevalence come from the increasing availability of information about autism on the internet and the increasing social awareness of the autism spectrum. Parents are becoming more alert to early childhood developmental issues and seeking evaluation earlier and more readily. The stigma often associated with autism in the past is declining. In addition, young adults with ASD are finding support groups through social media and those who need only minimal support are finding autistic mates on dating apps. Approximately 75% of autistic adults express a desire for a romantic relationship and 31% of autistic adults without intellectual disabilities are married. We will see in Section V that genetic predisposition is a critical element in the occurrence of ASD. So as more and more autistic adults marry and have children, that social development can lead to an increase in incidence of autism among the next generation. The chances of passing along genes favoring autism is, of course, greater for marriages involving two autistic partners. But such marriages appear to be among the most successful for people on the autism spectrum: autistic-autistic couples have a divorce rate 10% lower than that for autistic-neurotypical couples.
The changes in diagnostics, screening practices, public awareness and social acceptance of ASD, and the increasing rate of autistic adults having children who are often themselves on the spectrum, may in combination explain all of the rapid rise in apparent prevalence seen in Fig. I.1. Certainly, these changes leave only little room for an actual increase in incidence caused by environmental toxins, pharmaceuticals, or whatever other chemicals Robert F. Kennedy, Jr. seeks to blame for the rise in prevalence. His characterization of the rise as an “epidemic” caused by an “environmental toxin” is a scare tactic unsupported by honest analyses, introduced to search for scapegoats, rather than for understanding.
III. Alleged causes of autism: blaming the moms
It can be stressful for parents who are raising autistic children. After the discovery of autism in the 1940s, researchers devoted a great deal of time to discovering the cause of this condition. From about 1940 to 1960, psychoanalysis played a major role in analyzing behavior, while genetics was still in an early stage. Thus, Freudian analysts initially played a dominant role in suggesting causes and treatments for autism. Unfortunately, analysts generally suggested that autism resulted from malignant parenting; in particular, analysts claimed that autism was the result of mothers who neglected their children and provided them with little warmth or affection. We call this phenomenon “blaming the Moms.” It was devastating for mothers dealing with the challenges of raising autistic children to be told that not only were they responsible for autistic children, but that the most effective “remedy” was to remove the children from their mothers. Now that we know that a dominant cause of autism is genetics, we can appreciate the extremely damaging effects of blaming the Moms.
In this Section, we will focus our attention on three individuals who claimed that mothers were responsible for their autistic children. We review the careers of Bruno Bettelheim and Alice Miller, and we show how they attributed the behavior of mentally challenged children to neglect or abuse by their parents. A third case that we treat is current Secretary of Health and Human Services Robert F. Kennedy, Jr. In his case he claims that the “epidemic” of autism must be the result of toxic chemicals. Starting in Sept. 2025, Kennedy claims that a major cause of autism is acetaminophen (sold as Tylenol in the U.S.) taken by mothers during pregnancy. Once again, the (false) implication is that these mothers have caused their child’s autism by taking Tylenol. So we consider this to be another case of “blaming the Moms” for their child’s autism.
A: The Devious Bruno Bettelheim
Most of the world knew of Bruno Bettelheim as the Viennese scholar and intellectual who for three decades headed the Sonia Shankman Orthogenic School at the University of Chicago. Bettelheim, who is shown in Figure III.1, was a Freudian analyst who believed that children with behavioral disorders could be “cured” by extensive psychoanalytic therapy. Bettelheim made several appearances on television, particularly on the Dick Cavett Show, where he discussed his work with disturbed children. He maintained that, through psychoanalysis, he was able to provide these children with extensive personalized treatment that enabled them to live satisfying lives and overcome their difficulties. Bettelheim insisted that the children he treated, including many autistic children, were not born that way but had suffered emotional trauma that handicapped them.

Bettelheim also engaged in Freudian analyses of children’s fairy tales, particularly those of the Grimm Brothers. In 1976, Bettelheim published a Freudian analysis of fairy tales in his book The Uses of Enchantment: the Meaning and Importance of Fairy Tales. The cover of this book is shown in Figure III.2. In this book, Bettelheim argued that dark fairy tales such as those published by the brothers Grimm that described abandonment, grief and stress were references to childhood traumatic experiences. Children could relate the childhood trauma described in these folk tales to their own suffering, and with assistance from psychoanalysts could recover to pursue normal lives. The Uses of Enchantment brought fame to Bettelheim, winning the National Book Critics Circle Award for Criticism and the National Book Award in the category of Contemporary Thought. It cemented his reputation as a public intellectual and as a perceptive healer of distressed children.
It is no wonder that Bettelheim enjoyed a great reputation during most of his life. This erudite and persuasive Viennese psychiatrist claimed three doctoral degrees – one in art history, a second in philosophy, and a third in psychology, each achieved summa cum laude. To cap it off, Bruno had a personal recommendation from Sigmund Freud himself. Bruno Bettelheim’s personal history also gave enhanced credence to his psychoanalytic theories. Bettelheim was born to a family of Austrian Jews. In May 1938 he was arrested by Nazi authorities and imprisoned in the Dachau and Buchenwald concentration camps. However, in April 1939, Bettelheim was released as part of a prisoner amnesty declared for Hitler’s birthday. He claimed to have interviewed 1,500 people who had been imprisoned in concentration camps as part of his psychological investigations. And he used insights gained from observing his imprisoned colleagues to inform his treatment of disturbed children.
Bettelheim became known as a world expert in the causes and treatment of autism. Since he rejected the idea that autism was an inherited neurodevelopmental condition, he believed that autistic children had been terrified by events in early childhood. And he fixed on a theory that had been floated by Leo Kanner, the Austrian-American physician who was among the first to diagnose the condition of autism. Although Kanner had originally maintained that autism was innate, later in his life he observed that a number of the mothers of autistic children seemed to share common traits. He described his observations in a 1949 paper, where Kanner outlined some general observations regarding the mothers of autistic children. Many of the mothers were women of above-average intelligence who had professional careers, who devoted relatively little time to interacting with their children, and whose interactions with their autistic children showed relatively little affection. Kanner speculated that the “obsessive preoccupations and remarkable memory feats” of these children represented “a plea for parental approval.” Kanner remarked about these autistic children. “They were kept neatly in refrigerators which did not defrost.”
To be fair to Kanner, his work on autistic children was ground-breaking. He described the features of autism, gave it a name, and differentiated it from childhood schizophrenia. In his early work with autistic children, he emphasized that the features of autism seemed to be present at birth. So his later suggestion that autism was a response to the lack of affection from their mothers was a departure from his previous research. However, the depiction of autism as a response to “refrigerator mothers” caught on with psychoanalysts, and notably with Bruno Bettelheim. Since Bettelheim refused to acknowledge that autism might be a neurodevelopmental disorder, he seized on the argument that the cause of autism was due to a lack of emotional warmth, and in particular was a failure of the mother to provide the child with sufficient love and attention. Bettelheim was sufficiently articulate on this point that the “refrigerator mother” hypothesis is often called Bettelheim’s theory of autism. Blaming the mother for the behavior of autistic children was par for the course at this time. In her book Autism, Lisa Benaron argues “Although it now seems beyond comprehension that anyone would believe that autism is caused by deep-seated issues arising in early childhood relationships, virtually every psychiatric condition was attributed to parent-child relationships in the 1940s and 1950s, when Freudian psychoanalytic theory was in its heyday.”
As Director of the Sonia Shankman Orthogenic School at the University of Chicago, Bruno Bettelheim put his theories into practice. Since he theorized that the mother was the cause of autistic behavior, Bettelheim insisted on having these children reside at his school, claiming that the children would benefit from a “parentectomy.” He also claimed an exceptionally high success rate for the children in his school – he argued that in 43% of the children in his school, his methods resulted in a successful transition to normality for these students. And he claimed that many of his methods for treating autistic children were derived from his observations of his fellow inmates in Nazi concentration camps.
During the 30 years when he was Director of the Chicago Orthogenic School, Bettelheim was lauded as a brilliant clinician who achieved wonderful success working with emotionally disturbed children. This apparently incredibly gifted individual managed to blend his knowledge of childhood literature, psychology and philosophy into a treatment program for these children. Millions of people would see Bettelheim’s appearances on the Dick Cavett Show and be dazzled by his wide-ranging erudition.
However, the methods of Bettelheim and other psychoanalysts were incredibly damaging to the mothers of autistic children. The behavioral problems of autistic children would arise gradually; in many cases, otherwise extremely intelligent individuals would never develop interpersonal skills, and they would engage in repetitive, solitary behavior. So, parents of autistic children would be extremely anxious as these behaviors were manifested. However, the psychoanalytic theories blamed the condition on the actions of the parents, and particularly the mothers. For a mother to be told that her deficient parenting was the cause of this condition must have been excruciating. For professional women, the explanation was that she had abandoned her God-given role as a mother in favor of a selfish attachment to her own career. The criticism that a career interferes with a woman’s “natural role” as a mother is even today a staple of religious conservative thought. Bettelheim further accused the mother that “the precipitating factor in infantile autism is the parent’s wish that his child should not exist.” What a monstrous accusation to hurl at the mother, who is already dealing with the perplexing behavior of her child. And the subsequent diagnosis that the child could only heal if it was removed from her mother would be exceptionally cruel, especially as we now realize that the “refrigerator mother” origin of autism was entirely bogus.
Bettelheim Unmasked:
Our current understanding of Bruno Bettelheim represents a 180o shift from his earlier lofty reputation. Much of this is gleaned from biographies of Bettelheim by people like Nina Sutton (Bruno Bettelheim: The Other Side of Madness, 1995, shown in Figure III.3), and Richard Pollak (The Creation of Dr. B: A Biography of Bruno Bettelheim, 1997, shown in Figure III.4). These books discuss the fact that Bettelheim’s Freudian theories of the origin of autism were completely wrong, as we now know that autism is caused by neurodevelopmental issues and is present at birth. But more than that, Bettelheim’s entire life history is largely false. A review of Pollak’s biography from the Chicago Tribune concludes that “Bettelheim was a snake-oil salesman of the first magnitude.”

Let’s first review Bettelheim’s claim that he had doctoral degrees in art history, psychology and philosophy. It appears that Bettelheim possessed a degree in art history, although it is not clear it was a doctorate. As for the doctoral degrees in psychology and philosophy (summa cum laude doctorates, according to Bettelheim), biographers were able to find a maximum of three introductory courses in psychology. Furthermore, during the 14 years that Bettelheim claimed to be at university working on his many doctorates, he was in fact working in his family’s lumber business!
Bettelheim was one of many immigrants who escaped Nazi-occupied Europe in the 1930s. He used his arrival in the U.S. as an opportunity to reinvent himself. When he arrived in the U.S. and was hired as an assistant to Ralph Tyler at the University of Chicago, Bettelheim claimed, falsely, that he had extensive training in psychology and experience in treating autistic children; in addition, he claimed to have experience working with well-known psychoanalysts and had a favorable recommendation from Sigmund Freud. “This is exactly the person we need for psychoanalysis to grow and develop,” Bettelheim reported that Freud said of him – but apparently Bettelheim never met Freud. There is no evidence that he had any of these qualifications or experience in psychoanalysis. Also, Allen Dundes alleged that Bettelheim’s highly acclaimed Freudian analysis of fairy tales, The Uses of Enchantment, had copied extensively from a 1963 book by Julius Heuscher, A Psychiatric Study of Fairy Tales.
Bettelheim first gained attention in 1944 when he published an account of his observations of concentration camp prisoners, “Individual and Mass Behavior in Extreme Situations.” He alleged that in order to cope, concentration camp prisoners essentially reverted to child-like behavior. Bettelheim claimed that his observations were based on interviews with 1,500 concentration camp prisoners in five barracks. But accounts of his life in the Nazi camps show that he only ever lived in two barracks, so there is no way he could have interviewed that many people. Interestingly enough, in his accounts of childhood autism, Bettelheim turns his concentration camp theory around and claims that in order to deal with their childhood traumas, these autistic children behaved like prisoners.
Since we now know that autism is a neurodevelopmental disorder and not the result of terrible parenting, people have examined Bettelheim’s methods of treatment and his reports of success. Once again, Bettelheim constructed a wildly exaggerated account of his methods. As one example, despite his self-styled reputation as a witty and perceptive genius who treated his youthful patients with the most gentle and encouraging methods, Bettelheim had a fierce temper, and he took out his tantrums on staff and children alike. According to Pollak, one counselor at the Chicago Orthogenic School referred to Bettelheim’s methods as the “Nazi-Socratic Method;” and counselors in the Chicago area are said to have referred to him as “Brutalheim.” Bettelheim described his philosophy of child-rearing as being incredibly warm and supportive, and he claimed that coercive methods should never be used with children. However, he regularly spanked or slapped children or staff at the school; and a few women stated that in reassuring them after having struck them during a tantrum, he would fondle their breasts.
Today no one would be able to claim this tremendous success rate in applying Freudian techniques to deal with autistic children. Therefore, a number of contemporary critics have questioned whether the children at the Chicago Orthogenic School were actually autistic. It would seem that either the diagnosis of autism was incorrect for many of these children, or else Bettelheim’s claimed success rates were just another of his many shameless embellishments.
Starting in the 1960s and continuing through the 1970s, it was shown conclusively that autism was a neurodevelopmental disorder and not the result of bad parenting. To Bruno Bettelheim’s shame, he never acknowledged that this modern theory of childhood autism was correct, and therefore his psychoanalytic theories blaming the mother were simply false. In 1990 Bettelheim, suffering from depression and a number of physical ailments including a stroke, took his own life. He went to his grave having never publicly disowned his discredited theory, nor having acknowledged the harm that his “refrigerator mother” diagnoses had done to so many parents of autistic children.
In the interest of fairness, we want to acknowledge that the Bettelheim biography by Richard Pollak is in part a revenge story. Pollak’s younger brother Stephen had been a patient for five years at Bruno Bettelheim’s Chicago school. While playing at home on a vacation, Stephen had fallen from a hayloft onto a concrete floor and died. Richard Pollak visited Bettelheim in an attempt to obtain information about his brother’s life at the Orthogenic School. He was astonished when Bettelheim claimed that his mother had rejected Stephen at birth, causing his autism; and he asked Richard “What is it about these Jewish mothers?” Bettelheim further insisted that Stephen had committed suicide. None of Bettelheim’s claims resonated with Richard. He knew his mother as loving and caring; furthermore, his brother had fallen through a chute that was covered with hay, and it seemed extremely unlikely that he had deliberately fallen to his death.
Since Bettelheim had made allegations that RIchard Pollak knew to be untrue, he began to investigate other claims Bruno had made. Pollak’s resulting biography is an unsparing account of the lies from the renowned psychoanalyst. Many reviewers have noted the bitter tenor of Pollak’s book; however, they have found that facts alleged by Pollak are generally corroborated by people who knew Bettelheim well.
B: The Influential Alice Miller
Alice Miller (January 1923 – April 2010) was a Swiss psychologist, who became one of the most influential analysts and philosophers of her time. Miller’s own life was filled with drama. She was born Alicja Englard in Poland, the oldest daughter in an Orthodox Jewish family. Her family then lived in Berlin until 1933, but they returned to Poland after the Nazis seized power in Germany. In 1939 the Germans confined all Jews in the ghetto of her hometown Trybunalski. At age 16, Alice changed her name to Alice Rostowska and managed to smuggle her mother and sister out of the ghetto. For a while they hid in a Catholic convent in Warsaw, but Alice’s mother wanted the family to move to an apartment. Alice answered an ad for an apartment; however, the man who placed the ad was a szmalcownik, a Gestapo agent named Andrzej Miller. Miller made a living by blackmailing Jews, threatening to turn them into the Nazis, or by blackmailing Poles who aided Jews. When Alice realized her family’s peril, she seduced Miller and married him. They had two children and eventually moved to Switzerland, where they eventually divorced. Figure III.5 is a photo of Alice Miller.
Alice Miller studied psychoanalysis and from 1960 to 1980 she practiced it in Zürich, Switzerland. However, she then rejected both Freudian and Jungian psychoanalysis. She began to articulate her own theories of the behavior of disturbed children. Dr. Miller claimed that many children repressed their memories of abuse from their parents. In addition to the normally accepted examples of parental abuse, Miller added actions like corporal punishment, or even leaving infants to cry to avoid “spoiling” them. Miller claimed that these children would wall off their memories of being abused. However, this unresolved history of childhood abuse would then recur when these children became parents. Miller pointed to cases where people who had been abused would mistreat their own children in the same way that they had been abused.
Miller also claimed that she could trace abusive situations such as war or terrorism or even religious cults back to a person’s unresolved childhood abuse. She also linked personal afflictions to abuse of children by their parents. For Miller, instances of depression, eating disorders or addiction were all the result of the repression of parental abuse that people had suffered as children. Apparently, Alice Miller had much success in helping people remember instances of abuse, understanding how this had affected their subsequent development, and developing beneficial ways of dealing with their issues. She authored several best-selling books outlining her theories and her methods for helping her clients to move forward in healthy ways. Books such as The Drama of the Gifted Child (shown in Fig. III.6) and Thou Shalt Not be Aware: Society’s Betrayal of the Child won major awards, and Miller influenced an entire generation of analysts.
However, when it came to people with autism or other neurodevelopmental disorders, Miller’s theories failed. Her insistence that the behavior of autistic children was the result of parental abuse was just as wrong as Bettelheim’s insistence that autism was caused by “refrigerator mothers.” In fact, all psychoanalytic theories that attribute the behavior of autistic children to issues of bad parenting will fail to address the real issues. An interesting book that touches on these issues is Pluto’s Republic, a 1982 collection of essays by Sir Peter Medawar. Medawar shared the 1960 Nobel Prize in Physiology or Medicine for his discovery of acquired immunological tolerance and also for his skin grafting techniques, which led to the field of organ transplantation. Medawar was also a philosopher of science, and the collected essays in this book included extensive discussions of science vs. pseudoscience. Medawar was extremely critical of Freudian psychology. In one essay he recounted horrific stories of cases where Freudian analysis of genetic disorders led to ineffective and even harmful treatment. Medawar suggests that most, if not all, behavioral disorders will eventually be linked to neurological origins. While this likely represents an overstatement, in the case of autism it is certainly true that Freudian analysis of autistic children totally failed to identify the cause of this condition.
C: Tylenol and Autism
After Robert F. Kennedy, Jr. was confirmed as Secretary of Health and Human Services, in April 2025 he announced at a Cabinet meeting that he was launching “a massive testing and research effort” to find the cause of autism. He announced that this effort “will involve hundreds of scientists from around the world. By September [2025] we will know what has caused the autism epidemic and we’ll be able to eliminate those exposures.” All of Kennedy’s assertions about autism were problematic. First, as we have reviewed in previous sections, the increase in diagnoses of childhood autism does not reflect a recent “massive epidemic” of autism. There are several factors responsible for increased autism diagnoses. First, at present we have greater awareness of the disorder and are better able to identify cases of autism. Second, we now recognize an “autism spectrum disorder” or ASD, ranging from the mildest cases such as Asperger’s syndrome where the patients are often significantly above average in intelligence and are able to lead rather normal lives, to the most severe cases where patients need constant care over their lifetime. These factors play a major role in the increasing frequency of ASD that is currently reported.
RFK Jr.’s insistence that autism is caused by exposure of the mother to environmental chemicals flies in the face of scientific evidence. As we will show in Section V, a major factor in ASD is genetics, a fact which Kennedy has never acknowledged. Comparison of autism in identical twins and fraternal twins is one source of evidence that demonstrates the importance of genetic factors in the autism spectrum. A large number of different genes are often involved in ASD. There are also possible additional factors such as viral infections, medicines, exposure to environmental chemicals, or complications during pregnancy.
As we mentioned in the Introduction, on Sept. 22, 2025, Donald Trump and Robert F. Kennedy, Jr. held a press conference to announce an association between women taking Tylenol (see Fig. III.7) during their pregnancy and the occurrence of autism in their child. The claims in the press conference were mainly based on a study by a group led by Harvard University researchers. They analyzed the results from 46 earlier studies that looked for associations between the use of acetaminophen (known in the U.S. under the brand name Tylenol and elsewhere as paracetamol) and the occurrence of neurodevelopmental disorders (NDDs) such as autism or ADHD. Since Tylenol is available as an over-the-counter pharmaceutical and often not prescribed, many of the earlier studies have had to rely on women’s recollection of how much acetaminophen they had taken during their pregnancy. Andrea Baccarelli of the Harvard T.H. Chan School of Public Health was the lead author of the paper. The research team announced that their analysis of those 46 studies found an association between the use of acetaminophen by pregnant women and the occurrence of NDDs in their children. They concluded “We recommend judicious acetaminophen use — lowest effective dose, shortest duration — under medical guidance, tailored to individual risk-benefit assessments, rather than a broad limitation.”

However, there are robust data that reach the opposite conclusion – that there is no association between NDDs and acetaminophen exposure before birth. That comes from a 2024 study funded by the U.S. National Institutes of Health that examined data for 2.4 million children born in Sweden. This was by far the largest cohort of children that have been studied. When the researchers first examined the data, there seemed to be a slight increase in risk of NDDs for women who took acetaminophen during pregnancy. However, since the researchers had access to such a large cohort, they were able to separate out cases where a woman had two children, and who took differing amounts of acetaminophen in the two pregnancies. The researchers could compare the two cases to see if increased amounts of acetaminophen corresponded to an increased risk of NDDs. In those cases, researchers found no association between amounts of the drug and the incidence of NDDs.
Next, what does it mean if there is an “association” between taking Tylenol during pregnancy, and the risk of the child having a neurodevelopmental disorder? We should emphasize that finding an “association” is very different from concluding that taking Tylenol caused the NDD. As people have pointed out, there is an association between eating ice cream and shark attacks – both of those increase during summer months (more people are swimming during the summer when the water is warmer). But no one would conclude that eating ice cream causes shark attacks. People take Tylenol because of pain or fever; so, taking Tylenol is associated with decreasing pain or fever during a pregnancy. We know that NDDs can be influenced by stresses such as pain or fever during pregnancy. So, it is possible that the risk for NDDs was increased by health complications in pregnant women, and that those health complications were associated with Tylenol use.
The take-away is that pregnant women should consult with their doctors to see if taking Tylenol is recommended for pain or fever; and Tylenol should be taken in moderation. People should be aware that there is no direct evidence that taking Tylenol causes autism; it is even uncertain whether there is an association between taking Tylenol and the occurrence of autism. However, this is completely different from the message given by Donald Trump in his Sept. 22 press conference.
The video linked below shows the full hour-long Sept. 22 press conference. Trump opens with remarks followed by Robert F. Kennedy, Jr., Jay Bhattacharya and others. We are most interested in the remarks made by Trump in the first 12 minutes of the press conference.
https://www.youtube.com/watch?v=jcMWxMetMHo
Trump first begins by drastically over-estimating the rise in cases of autism since its discovery in the 1940s. As discussed earlier, diagnostic methods improved so that many more cases of autism were identified (in earlier days, autism may have been misdiagnosed as schizophrenia or some other mental illness). In addition, the definition of autism broadened dramatically to include non-profound cases of autism. Figure III.8 provides the definition of profound autism; it also claims that most studies of autistic children exclude those with profound autism from their participants. Figure III.9 shows the increase in autism rates from 2000 to 2016. This figure tracks the number of autistic 8-year-old children in every 1,000 children. It divides the autism diagnosis into profound and non-profound cases of autism. The definition of profound autism is that the child has an IQ of less than 50, or that the child is non- or minimally verbal (this is Level 3 autism as defined in Figure II.3).


Over this 16-year period, the number of profound cases of autism has increased from 0.27% in 2000 to 0.46% in 2016. During that same period, the number of non-profound cases has increased from 0.39% to 1.1% of the population. In both cases the incidence of autism increased substantially over a 16-year period; however, the rate of non-profound cases of autism increased significantly faster than the rate of profound cases. In an April 16, 2025 press conference, HHS Secretary Robert F. Kennedy, Jr. claimed that “autism destroys families,” and “is an individual tragedy as well.” Kennedy also made the false statement that many autistic children were “fully functional,” but “regressed … into autism when they were two years old. And these are kids who will never pay taxes, they’ll never hold a job, they’ll never play baseball, they’ll never write a poem, they’ll never go out on a date. Many of them will never use a toilet unassisted.”
Kennedy added “Most cases are now severe. Twenty-five percent of the kids who are diagnosed with autism are nonverbal, non-toilet-trained, and have other stereotypical features.” His remarks were based on the CDC study quoted in Fig. III.8; however, that study was on the high side of estimates of the fraction of profound autism cases. For example, a 2024 study by researchers at the University of Utah and Children’s Hospital of Pennsylvania studied 1,368 American autistic children. Asked if they would describe their child’s autism as “severe,” 10.1% of parents responded “yes.” And only 38% of those “severe” autism cases were said to have a “severe” intellectual disability. Furthermore, Fig. III.9 shows that Kennedy’s statement that “Most cases are now severe” is at odds with both data and the expanding diagnostic criteria discussed in Section II.
The vast majority of people on the autism spectrum do not have such extreme limitations. It is true that autism cases have been rising. But RFK Jr. has also greatly overemphasized the true numbers of this expansion. And then, when Donald Trump gets hold of the statistics, as shown in the YouTube video above, the numbers veer off into the truly fantastic. Trump estimates the increase as going from 1 case of autism for every 20,000 people to 1 case in every 12 people, in a period of about 25 years. But the rate of autism in 2000 was more like 1 in 150, and the current rate of ASD is roughly 1 in 31. (Note: Figure II.6 demonstrates that the rate of ASD varies significantly from state to state, most probably as a result of different evaluation and testing practices.) This extreme estimate of the rise in ASD cases allows Trump to describe the situation as “probably the largest increase ever” in any condition. This claim is in line with RFK Jr.’s repeated insistence that autism rates have become “an epidemic” and therefore must be caused by environmental chemicals whose use has been increasing lately.

There is no evidence that taking Tylenol causes autism. But Trump’s Sept. 22 message was shockingly different, and contradictory to the best scientific evidence, as shown by Figure III.10, where Trump’s claims were fact-checked by NPR. “Tylenol is not good,” he stated. It should only be taken by pregnant women who “can’t tough it out,” but if possible they should avoid taking it altogether. “There is no downside” to avoiding Tylenol during pregnancy, he claimed. This statement is absolutely false. Tylenol can help relieve fever and pain, and we know that fever and pain can be associated with an increased risk of an NDD. In addition, based on no medical advice, Trump stated that children less than one year old should not be given Tylenol “for virtually any reason.” The American Academy of Pediatrics says that acetaminophen is safe for young children to use to treat fevers, although children under 12 weeks old should only be given that medication when directed by a doctor. Figure III.11 shows a BBC article from Sept. 23, 2025 fact-checking the many false and misleading statements that Donald Trump made in the Sept. 22 press conference on autism.

Trump also repeated a persistent myth that there are no autistic children in Amish communities. The Amish do have autistic children. The numbers seem to be about one-third of the rate of autism in the general public; however, that may be due to differences in the way Amish report cases of autism. The claim that the Amish have no cases of autism is related to the myth that no Amish are vaccinated. In fact, many Amish are vaccinated, although vaccination rates differ in various Amish communities. Another myth is that the Amish don’t take any medicines and as a result, they rarely get any diseases. The fact is that Amish communities are so inbred that they experience genetic conditions that are unknown outside of their own communities. Furthermore, various Amish groups take medications including Tylenol. Trump also repeats the myth that the Cubans can’t afford Tylenol, and as a result they have no autism. In fact, the Cubans do have autism. Furthermore, although there are sometimes shortages of that medicine, acetaminophen is available in Cuba. Reporting and testing methods are more sporadic in Cuba, so the level of autism is not accurately known. But the Cubans recognize autism spectrum disorder and are taking steps to provide diagnosis and treatment for autistic children.
There is no doubt that Robert F. Kennedy, Jr. is the worst Secretary of HHS in our country’s history. He lies constantly and goes to great lengths to repeat falsehoods about the causes of autism, the dangers of vaccination, and he also pushes dubious remedies to deal with diseases like measles. But the combination of RFK Jr. and Donald Trump is simply lethal. Trump receives misinformation and conspiracy theories from RFK Jr. and others, and he then exaggerates these myths to fantastic lengths. Furthermore, Trump’s expressed belief that he is “always right” convinces his MAGA supporters to take seriously his wacky notions. On the basis of Trump’s press conference covered in the YouTube video above, we can expect that many Americans will be convinced that Tylenol causes autism. He mused about the “beautiful babies” whose lives were ruined because they were “pumped full” of “enough vaccines for a horse.” We will discuss Trump’s misinformation about vaccines in the next section.
However, the combination of Trump’s statements at his press conference and Robert F. Kennedy’s assertion that they have uncovered a chemical that causes autism will cause tremendous confusion in the American public. People who believe Trump will take his wild assertions for gospel; they will badger their OB/gyn doctors, and they may well take Trump’s word over assertions by the pharmaceutical companies and their own doctors. The Trump press conference was widely reported on. Figure III.12, taken from a KFF tracking poll after the Trump-Kennedy press conference, shows that the vast majority of Americans heard the Tylenol-autism claim. Roughly equal numbers of men and women, and Republicans and Democrats, heard these claims.

In a recent post, we discussed significant differences in health treatments and outcomes between Red and Blue states. The claims by Trump and Kennedy regarding autism and vaccines will only serve to exacerbate these differences. MAGA supporters, more numerous in Red states and rural areas, will be more receptive to the health misinformation from these two. Thus, we will expect to see fewer expectant mothers taking Tylenol in pregnancy in Red states. They will not relieve a fever by taking Tylenol. But since fevers during pregnancy are associated with increased incidence of autism, this will quite likely increase rates of autism there. We may also see increased instances of medical professionals leaving Red states, as they encounter more and more resistance to their recommendations from their patients. Figure III.13 bolsters our claims. Although nearly two-thirds of all Americans rated the claim that taking Tylenol increases the risk of autism as “probably false” or “definitely false,” 57% of Republicans said that the claim was “probably true” or “definitely true.” Thus, we can expect differences in health-care outcomes between Red states and Blue states to widen.

Most recently, RFK Jr. has tried to bolster his claims about a Tylenol-autism risk by invoking yet further dubious studies. During a Cabinet meeting on Oct. 9, 2025 he asserted: “There’s two studies that show children who are circumcised early have double the rate of autism. It’s highly likely because they are given Tylenol.” First of all, neither of the referenced studies had evidence that acetaminophen was given to the boys being circumcised. The 2015 study found an enhancement in the autism risk of circumcised boys under age 5, but no statistically significant enhancement after age 5. Since autism does not disappear on its own, the study’s findings are inconclusive. The 2013 study compared circumcision and autism rates in eight countries. But, as Dr. Céline Gounder points out: “Circumcision practices are also tied to culture and religion, which also affect autism diagnoses and healthcare use.” Both of these studies are inconclusive even about an association of autism with circumcision, let alone a causal relationship or a tie to acetaminophen. Neither would be worth referencing unless one is looking for any evidence to support a conclusion already based on flimsy other evidence.
And finally, the Tylenol-autism claims represent yet another example of “blaming the Mom” for their child’s condition. A mother who took Tylenol during pregnancy and who gives birth to an autistic child, and who believes the falsehoods spread by Kennedy and Trump, will necessarily feel that she is responsible for this outcome, because she was not able to “tough it out” and refrain from taking this medication, even if her doctor recommended it.
— Continued in Part II —
